ℹ️ Skipped - page is already crawled
| Filter | Status | Condition | Details |
|---|---|---|---|
| HTTP status | PASS | download_http_code = 200 | HTTP 200 |
| Age cutoff | PASS | download_stamp > now() - 6 MONTH | 0 months ago |
| History drop | PASS | isNull(history_drop_reason) | No drop reason |
| Spam/ban | PASS | fh_dont_index != 1 AND ml_spam_score = 0 | ml_spam_score=0 |
| Canonical | PASS | meta_canonical IS NULL OR = '' OR = src_unparsed | Not set |
| Property | Value |
|---|---|
| URL | https://www.cognitivefxusa.com/blog/fast-acting-depression-treatment-options |
| Last Crawled | 2026-04-12 05:08:02 (7 hours ago) |
| First Indexed | 2024-08-20 00:39:55 (1 year ago) |
| HTTP Status Code | 200 |
| Meta Title | Fast-Acting Antidepressants: Compare Options & Effectiveness |
| Meta Description | Learn about fast acting depression treatments, including TMS and ketamine. View their effectiveness, side effects, and how they work. |
| Meta Canonical | null |
| Boilerpipe Text | Compare the Top Fast-Acting Depression Treatments: Effectiveness, Time Frames & Side Effects
•
Updated on 31 March, 2026
•
Traditional antidepressant medications involve a trial period of weeks or months before it can be determined whether or not they are working. If a medication doesn’t work — and it’s been
shown
that
traditional antidepressant medications only work for about one-third of patients
— then the patient must begin another trial with a different drug and go through the process all over again.
Throughout these trials, patients often experience unpleasant side effects that
impact
their quality of life. And beyond a second failed antidepressant drug, data
suggests
that less than 2% of patients have success with a third or fourth medication.
Patients need new treatment options that help relieve their symptoms faster, ideally with fewer side effects. In this article, we discuss what’s available at the moment, including:
Transcranial magnetic stimulation (TMS)
Ketamine
Esketamine
Dextromethorphan-bupropion
Transcranial Magnetic Stimulation (TMS)
TMS is a noninvasive, FDA-approved procedure that uses magnetic pulses to restore normal activity levels in a part of the brain called the dorsolateral prefrontal cortex (DLPFC) which is consistently
affected
by depression and other mood disorders. During a TMS session, an electromagnetic coil is placed over the patient’s head directly above the DLPFC, and pulses are applied at specific intervals to stimulate nerve cells in that area.
Patients who receive newer forms of TMS can experience relief from their depression in a single week of treatment. TMS also has mild
side effects
compared to antidepressant medications which we’ll discuss below.
Types of TMS
Repetitive Transcranial Magnetic Stimulation (the Original Method of TMS)
The original form of TMS was first
used
in the treatment of depression in the mid-90s. This procedure — called
repetitive transcranial magnetic stimulation (rTMS) —
involves
the
application of
repeated
electromagnetic pulses delivered by a magnetic coil placed on the patient’s scalp over the DLPFC area.
Usually,
patients
receive 20-30 TMS sessions, delivered daily over four to six weeks, with each
session
lasting up to 40 minutes.
Many
patients begin feeling better after just two weeks.
About 50% of patients
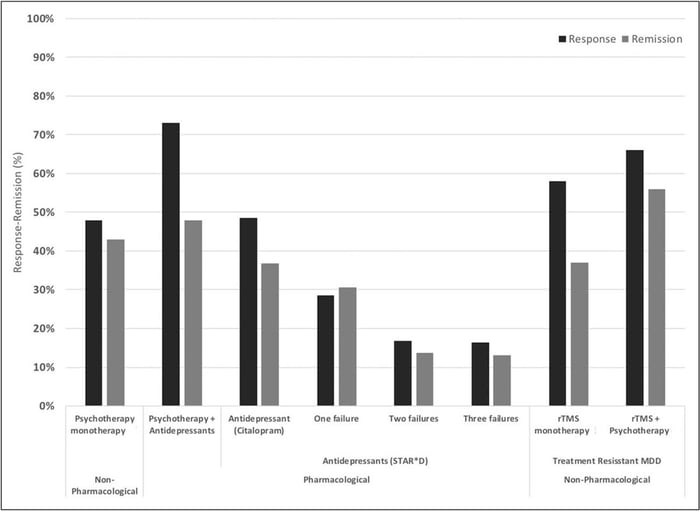
respond well to treatment with over 30% showing complete remission. When combined with psychotherapy, success rates are even more impressive with response and remission rates of ~66% and ~55% respectively.
Response and remission rates of various monotherapeutic and combinatory antidepressant treatments based on the largest studies and datasets available.
[Source]
Accelerated TMS (Reduces Treatment Time to a Single Week)
Showing up to daily sessions for four to six weeks has been impractical for many patients due to work and life commitments. To solve this issue, researchers developed
accelerated TMS
, where patients undergo multiple TMS sessions per day and can complete treatment in a single week.
Accelerated TMS is
as safe
as daily rTMS and potentially more effective. In addition, patients
receiving
multiple sessions each day seem to experience improvements in symptoms faster than those receiving daily sessions, and the effects are still
visible
months after their treatment.
Intermittent Theta-Burst Stimulation (a New Method of TMS)
In 2018, the FDA approved a new version of accelerated TMS called
Intermittent Theta-Burst Stimulation (iTBS)
. Theta waves are the frequencies the hippocampus uses to connect to other brain circuits and are utilized in memory formation, meditation, and certain phases of sleep. Theta burst stimulation uses a different magnetic pulse (in triplets) and delivers the treatment in three minutes (compared to 37 minutes in rTMS).
This method can produce rapid reductions in depression symptoms with many patients
experiencing
improvements shortly after starting their treatment. In addition, patients also noticed a decrease in
suicidal
ideation, suggesting that iTBS could be an option to rapidly treat patients at high risk of suicide.
fMRI-Guided iTBS (the Newest and Most Effective Method of TMS)
In the standard
rTMS and iTBS protocols
, the location to apply the coil is calculated based on taking manual measurements between the patient’s nose, ears, and top of the head. However, due to variations in head size and shape, or differences in brain organization between patients,
studies
have found this method of coil placement can be imprecise and lead to less consistent outcomes. Even missing the DLPFC by a few millimeters is enough to produce poorer results.
To overcome this limitation, researchers began using functional MRI and neuronavigation devices to determine exactly where the DLPFC is located in the depressed patient’s brain. This method, developed by a team from Stanford University, is known as the SAINT™ protocol. SAINT stands for Stanford Intelligent Accelerated Neuromodulation Therapy. The FDA
approved
SAINT depression treatment in September 2022, and it is now regarded as the “gold standard” treatment for treatment-resistant depression.
A comparison of remission rates for rTMS/iTBS, electroconvulsive therapy (ECT), and SAINT-iTBS.
The SAINT™ protocol involves 10 sessions per day over five days for 50 sessions total. In a double-blind randomized clinical trial,
about 85.7%
of patients responded to the SAINT-iTBS treatment
(meaning they met prespecified criteria for reduced depressive symptoms)
and around 78.6% met the remission criterion.
All the individuals in the study had treatment-resistant depression and had failed at least two other depression treatments.
One month after treatment, 60% were still in remission
.
The speed with which SAINT-iTBS can achieve high response and remission rates makes it one of the best rapid-acting treatments for depression available today. However, there is limited data on the durability of these outcomes and how well they hold up over time. Some patients see lasting remission or symptom reduction, while others need follow-up treatments to maintain the effectiveness. Studies show that TMS maintenance sessions can be extremely helpful, sometimes allowing patients to stay
symptom-free
for up to eight years.
In addition, combining TMS with cognitive behavioral therapy (CBT), as we do at our clinic, is likely to produce the best long-term outcomes for patients. While there are no studies yet combining iTBS and CBT, one
study
found that combining rTMS and CBT nearly doubled remission rates for patients.
Side Effects and Contraindications
TMS is a safe procedure with only
mild and short-lived side effects
, such as headaches, neck pain, or a tingling sensation in the scalp. These symptoms usually go away after a few sessions. The most serious complication is a seizure, but the risk is extremely low — less than 0.001% per session. Even if a seizure does occur, patients recover quickly and fully without any long-term effects.
TMS cannot be used if you have certain metallic implants or objects in your brain near where the coil is placed. This includes devices like cochlear implants, Internal Pulse Generators, medication pumps, aneurysm clips or coils, stents, or bullet fragments. However, braces and dental fillings are safe and won't interfere with treatment.
Some medications can increase the risk of seizures and might prevent you from having TMS. If you are on medication, it’s important to talk to your healthcare professional before starting TMS. For patients taking drugs with a high risk of seizures, TMS should be used with caution.
Receiving fMRI-Guided TMS at Cognitive FX
Our clinic in Provo, Utah, provides an alternative to SAINT™ TMS that offers
the same precision of personalized treatment targeting, combined with FDA-approved theta burst stimulation at a significantly lower cost.
This approach delivers the same core elements that make SAINT so revolutionary.
The only difference between our treatment and SAINT™ (a trademark licensed to Stanford Medical) is our targeting method. Our target locations are determined by fMRI and our prescribing neuroscientist and physician, rather than their proprietary software.
Comparison Chart
Accelerated fMRI - TMS vs. Magnus SAINT™ TMS
Accelerated fMRI - TMS
Magnus SAINT™ TMS
FDA-Approved iTBS
✔
✔
FDA-Approved Neuronavigators
✔
✔
FDA-Approved Figure 8 Coils
✔
✔
Number of Treatment Days
5
5
Treatments per Day
10
10
Total Treatments
50
50
Number of TMS Pulses
Approx. 90,000
90,000
Resting motor threshold pulse intensity
90–120%
90–120%
FDA-Approved Personalized DLPFC Targeting
✘
✔
Personalized DLPFC Targeting Assists Doctor in Target Location
✔
✘
Personalized E Field Coil orientation
✔
✘
Cost
$9,000 to $12,000
$30,000+
This accelerated protocol of iTBS is:
Safe:
Widely tolerated and associated with mild, short-lasting side effects.
Precise:
fMRI ensures that the treatment target area is precisely located for each patient, accounting for variations in head size and shape. Neuronavigation ensures the magnetic coil is placed over that exact spot for every treatment session.
Fast:
Treatment courses are reduced to a single week, making it easier to complete alongside life and work commitments (compared to 4 to 6 weeks of standard TMS and accelerated TMS protocols).
Effective:
Precision coil placement combined with theta burst stimulation produces the
best TMS treatment results to date
.
To improve patient outcomes, we also include cognitive behavioral therapy (CBT) as a part of our treatment. When combined with the traditional method of TMS (rTMS), CBT
improved response and remission rates
by ~8% and ~19%, respectively. Additionally, CBT is likely to produce sustained improvement over time once treatment has concluded.
Our brain stimulation treatment is ideal for most patients with treatment-resistant depression. However, we do not treat patients under the age of 18 or over 65. Additionally, as a safety measure, we do not treat patients who have a history of seizures or who are currently actively suicidal and in need of crisis care.
Click here
to learn more about receiving accelerated fMRI TMS therapy at Cognitive FX.
Other Fast-Acting Depression Medications for Treatment-Resistant Depression
Recent efforts to develop new pharmaceuticals for treating depression have primarily focused on increasing the levels of serotonin in the brain. However, the idea that depression is caused by low serotonin levels is still just a hypothesis.
Over the past three decades,
compelling
evidence has indicated that the neurotransmitter glutamate also plays a role in depressive symptoms. This research has enhanced our understanding of the brain mechanisms behind depression and has led to the development of new fast-acting antidepressants, such as ketamine, esketamine, and dextromethorphan-bupropion.
These antidepressants bind to N-methyl-D-aspartate (NMDA) receptors in the brain and block the activity of glutamate, an excess of which is thought to
contribute
to depression. However, glutamate is also an important neurotransmitter involved in memory and learning and is important for overall healthy brain function. By inhibiting it, some patients may
experience
cognitive impairments, a trade-off that patients should consider before starting any of these treatments. (TMS, in contrast, does not have this downside. Brain stimulation can
improve
the function of glutamate and other neurotransmitters and promote better brain function.)
Ketamine
Ketamine was approved by the FDA in 1970 to be used as an anesthetic. In 2000, a
clinical trial
showed that ketamine could be used to improve the mood of patients living with depression. Since then, multiple clinical trials have shown that ketamine is extremely fast-acting compared with traditional antidepressants and can
relieve
depressive symptoms, including
suicidal
ideation, for a period that can last days or weeks. Around
60%
of patients experienced the benefits of ketamine up to three days after a single treatment and about 40% of these patients still had not relapsed a month later. However, after six
months
and multiple ketamine treatments, only 26% of patients were still responding and only 15% were symptom-free and in remission.
In chemical terms, ketamine is a chiral molecule, meaning it has two chemical forms that are mirror images of each other: R-Ketamine and S-Ketamine. Racemic ketamine is a mixture of both R-Ketamine and S-Ketamine in equal parts and is the most commonly used form of ketamine in clinical settings.
Ketamine is administered to patients intravenously. During this procedure, patients are closely monitored by a healthcare professional because ketamine is a dissociative drug, which means patients can feel disconnected from reality and engage in dangerous and life-threatening behaviors. In addition, patients may also experience severe side effects, including:
Dissociation
Intoxication
Sedation
High blood pressure
Dizziness
Headache
Blurred vision
Anxiety
Nausea and vomiting
A typical treatment plan includes four to six sessions over two to three weeks. Some patients need booster sessions, typically once a month or once every three months, depending on the patient. To boost the effects of ketamine, it is recommended to combine it with a form of psychotherapy, such as cognitive behavioral therapy (CBT).
The surge in demand for this drug has paved the way for a cottage industry of clinics offering ketamine treatments. Some companies make sweeping claims that they’re able to treat dozens of conditions, including depression, anxiety, chronic pain, PTSD, bipolar disorder, and migraines. Such claims are currently not backed by scientific studies. As the industry is unregulated, the quality of care received at these clinics
can be highly variable.
Many clinics are not run by doctors of psychiatry and are simply pain management clinics that have added ketamine to their list of treatments or are spas with staff not trained in mental health treatment. In addition, it can be expensive. Typically, treatments cost between $400 to $1,000 per session, which can add up to thousands for the full treatment. If you’re considering this option, our advice is to discuss it with your family doctor before committing to any clinic.
Esketamine (Brand Name: Spravato)
Ketamine shows some promise in treating treatment-resistant depression, but the IV administration is time-consuming. To overcome these issues, researchers developed a new antidepressant using only the S-ketamine fraction, aptly named Esketamine. In 2019, the FDA approved this product as a nasal spray for easy application, sold under the brand name Spravato.
Clinical
studies
have shown that S-ketamine has fast antidepressant effects, with some patients reporting a reduction in symptoms
within
hours of administration. This is in contrast to traditional antidepressant medications that can take weeks or months to take effect. This makes it particularly beneficial for patients who have not responded to other treatments or are in urgent need of treatment due to severe suicidal tendencies. After an eight-week treatment,
about
one third of patients had achieved remission and, of these, about one third had not relapsed more than eight months later.
Spravato comes with specific guidelines for administration due to potential side effects such as nausea, headaches, dizziness, disorientation, and dissociation immediately after use. It must be administered at certified treatment centers under the supervision of a mental health care professional. Ideally, esketamine should be used in conjunction with a conventional antidepressant medication. The aim is to use esketamine for fast relief from depression symptoms until the other medication takes effect.
In most cases, patients receive esketamine twice a week for the first month, and then if patients improve, they continue to receive the drug at a lower frequency for a few weeks or months. Typically, this means treatments start as weekly, then drop to every two weeks, then monthly, etc.
Arketamine
Researchers have also tested the R-ketamine fraction — called arketamine — to treat major depression and other mental health conditions, but this drug has not received approval from the FDA yet.
Preliminary
results are encouraging, with antidepressant effects faster and longer than ketamine and fewer side effects, especially in terms of dissociation and hallucinations. Clinical trials are currently underway in the US and other locations around the world.
In addition to its antidepressant-like effects, arketamine may help treat patients with various neurological disorders, such as Parkinson's disease and multiple sclerosis. Moreover,
arketamine
has anti-inflammatory, bronchodilating, and neuroprotective effects, which means it could be a new
drug
for patients with neurological disorders and inflammatory diseases.
Dextromethorphan-bupropion (Brand Name: Auvelity)
A new fast-acting medication called Auvelity was just approved by the US Food and Drug Administration to treat patients with major depressive disorder (MDD). Auvelity is a combination of two already existing drugs: dextromethorphan and bupropion.
Dextromethorphan is commonly used in cough syrups to provide temporary relief from cough. Recent
research
showed it can also be used to alleviate depressive symptoms, but it’s metabolized very quickly in the body. Bupropion is an existing antidepressant medication, which also slows down the metabolism of dextromethorphan in the body. Staying in the body longer means the levels of drugs are more stable and can potentially help patients more.
A phase three
clinical trial
confirmed that Auvelity can improve symptoms of depression and a few patients started experiencing the benefits after just one week. After six weeks, over 50% of the patients responded to the treatment and were feeling better and 40% were in remission which is a slightly higher remission rate than for other types of antidepressant medications. Crucially, this
combination
works significantly better than bupropion alone. After six weeks, only about 40% of patients responded to bupropion in isolation, and less than 20% achieved remission.
Auvelity doesn’t have the same safety restrictions as ketamine, making it a much safer alternative. Typically, it has similar
side effects
and warnings compared to existing antidepressant medications, including dizziness, nausea, dry mouth, decreased appetite, and anxiety.
There is a risk that Auvelity may increase suicidal thoughts and actions in young adults, adolescents, and children. For this reason, it’s essential to pay close attention to sudden changes in mood, behavior, thoughts, feelings, or suicidal thoughts when taking this drug.
Additionally, Auvelity should not be taken by patients with a history of seizures, or eating disorders, or those taking other antidepressants like monoamine oxidase inhibitors, benzodiazepines, barbiturates, or anti-seizure medicines.
Additional Considerations Regarding Traditional Antidepressant Medications
As described earlier, most antidepressants take weeks or months for patients to begin experiencing the benefits (if they experience benefits at all). However, there is some
evidence
that a few antidepressants work faster in some patients but there are no reliable ways to determine which patients will respond faster. These include, for example, some selective serotonin reuptake inhibitors (SSRIs), serotonin-norepinephrine reuptake inhibitors (SNRIs), and tricyclic antidepressants (TCAs).
SSRIs and SNRIs aim to increase the levels of serotonin and norepinephrine in the brain. They’re often the first option primary care doctors prescribe because they generally cause fewer side effects. Patients may experience better quality of sleep, higher levels of energy, and increased appetite within the first 1-2 weeks after starting treatment. Improvement in these physical symptoms can be an important early signal that the medication is working. In most cases, severe symptoms may still need up to 6-8 weeks to fully improve.
Some common examples of these drugs include:
SSRIs
Citalopram (Celesta)
Fluoxetine (Prozac)
Sertraline (Zoloft)
SNRIs
Venlafaxine (Effexor)
Desvenlafaxine (Pristiq)
Duloxetine (Cymbalta)
Similarly to SNRIs, tricyclic antidepressants also aim to increase the levels of serotonin and norepinephrine, but they tend to cause more side effects. They’re typically only prescribed for patients who have tried other antidepressants without improvement. One example of a fast-acting tricyclic antidepressant is called desipramine, and
more
than 50% of patients experience significant improvements during the first week of treatment.
However, it is important to note that response times to antidepressant medications vary greatly from patient to patient, and it is crucial to consult with a healthcare professional to determine the most appropriate treatment approach for an individual’s specific needs.
Conclusion
The treatment landscape for depression is evolving, with new options providing faster relief and potentially fewer side effects compared to traditional antidepressant medications. Traditional medications often involve a lengthy trial period and can come with unpleasant side effects, with only about one-third of patients having reliable reductions in depression symptoms.
Among the newer treatments, TMS stands out for its noninvasiveness and rapid effectiveness. Accelerated fMRI theta burst stimulation, in particular, offers a significant advancement by using fMRI and neuronavigation for precise coil placement, leading to high response and remission rates within a single week of treatment. This method, available at our clinic, is among the most effective fast-acting treatments for depression, with the added advantage of not impairing cognitive functions.
Other fast-acting treatments like ketamine, esketamine, and dextromethorphan-bupropion provide rapid symptom relief by targeting neurotransmitters such as glutamate. However, these treatments can come with side effects that patients should consider carefully, and the effects of these treatments are often not long-lasting.
Ultimately, the combination of fMRI TMS with cognitive behavioral therapy (CBT) offers a promising solution for many patients with treatment-resistant depression. This integrated approach not only provides rapid symptom relief but also promotes sustained improvement in brain function and overall mental health.
If you are interested in receiving accelerated fMRI TMS therapy at Cognitive FX,
click here to learn more
and see if you’re a good fit for treatment.
Cited Research
A reanalysis of the STAR*D study’s patient-level data with fidelity to the original research protocol
Repetitive transcranial magnetic stimulation treatment for depressive disorders
Stanford Neuromodulation Therapy (SNT): A Double-Blind Randomized Controlled Trial
Antidepressant effects of ketamine in depressed patients
Efficacy and Safety of Flexibly Dosed Esketamine Nasal Spray Combined With a Newly Initiated Oral Antidepressant in Treatment-Resistant Depression: A Randomized Double-Blind Active-Controlled Study
About the author
Dr. Diane Spangler, Ph.D.
Dr. Spangler is a Clinical Psychologist with over 20 years of experience working in both clinical and academic settings. She earned her doctorate degree in Clinical Psychology at the University of Oregon followed by a Postdoctoral Research Fellowship in the Department of Psychiatry at the Stanford University School of Medicine. Dr. Spangler served as a Professor of Psychology at Brigham Young University for 15 years where she directed training in Cognitive Behavioral Therapy for the Clinical Psychology Doctoral Program, and conducted research on the etiology and treatment of depressive, anxiety, and eating disorders. She also served as a Visiting Professor in the Department of Psychiatry Cognitive Therapy Centre at Oxford University in England. Dr Spangler has authored over 60 publications and has lectured worldwide. She has received numerous awards for her collective work from the National Institute of Mental Health, the American Psychological Association, the International Association for Cognitive Psychotherapy, the Association for Behavioral and Cognitive Therapies, the Beck Institute, and the National Association of Professional Women. |
| Markdown | \<img height="1" width="1" style="display:none" src="https://www.facebook.com/tr?id=1056215754466548\&ev=PageView\&noscript=1"\>
 
###### 280 W River Park Drive Suite 110 Provo, UT
[\+1 385 446-4161](tel:+13854464161)
[hello@cognitivefxusa.com](mailto:hello@cognitivefxusa.com)
[](https://www.cognitivefxusa.com/)
[**Get Started**](https://cognitivefxusa.typeform.com/depression?typeform-source=www.cognitivefxusa.com)
- [Brain Injury Treatments](https://www.cognitivefxusa.com/treatment) 
### Your Treatment
[Post-Concussion Syndrome Treatment Our intensive EPIC program helps patients recover from symptoms that haven't responded to traditional care.](https://www.cognitivefxusa.com/treatment)
[POTS Treatment POTS treatment clinic using neurological retraining, vestibular recalibration & CO₂ therapy. 5-day intensive program in Utah.](https://www.cognitivefxusa.com/pots-treatment)
[Viral Brain Injury Treatment Long Covid-19, Post-Treatment Lyme, Encephalitis. We utilize cutting-edge treatments to help you regain function.](https://www.cognitivefxusa.com/viral-brain-injury)
[What does CFX do for PCS? Learn more about post-concussion.](https://www.cognitivefxusa.com/)
[Book Consult Schedule a 30-minute call with one of our doctors to see if CFX precision treatment approach is right for you.](https://cognitivefxusa.typeform.com/consult-intake)
[Pricing Pricing for each of our treatment packages and other important financial information.](https://www.cognitivefxusa.com/pricing)
[Learn about the Brain Scan fNCI Standard brain scans show structure. fNCI shows function. It's the difference between a "normal scan" and being able to see what is wrong and treat it.](https://www.cognitivefxusa.com/fnci-brain-scan-at-cognitive-fx-56-regions-measured)
- [TMS Treatments](https://www.cognitivefxusa.com/precision-mental-health-fmri-guided-transcranial-magnetic-stim) 
### Depression Treatment
[Depression Treatment fMRI Guided TMS Depression treatment with precision brain imaging meets advanced TMS protocols for depression that hasn't responded to medication.](https://www.cognitivefxusa.com/precision-mental-health-fmri-guided-transcranial-magnetic-stim)
[One-Day Depression TMS Treatment Protocol Accelerated depression treatment TMS protocol that compresses weeks of treatment into one day intensive session.](https://www.cognitivefxusa.com/one-d-tms-one-day-tms-accelerated-depression-treatment-protocol)
[Depression Treatment Resistant Quiz Tried multiple antidepressants with no relief? This free quiz evaluates your treatment history, symptoms, and risk factors to help you understand your next steps.](https://www.cognitivefxusa.com/treatment-resistant-depression-quiz-free-self-assessment-no-email)
[Schedule Consultation Schedule a 30-minute telehealth visit with our team to discuss potential TMS treatment.](https://www.cognitivefxusa.com/tms-consultation-signup)
[Depression Treatment Blogs Learn more about TMS treatment for depression. And how effective it can be for patients with treatment-resistant depression.](https://www.cognitivefxusa.com/blog/topic/transcranial-magnetic-stimulation-tms)
- [Treatment Results](https://www.cognitivefxusa.com/our-patients) 
### Patient Results
[Publications Learn more about post-concussion.](https://www.cognitivefxusa.com/our-research)
[Patient Results We see patients from all over the world with different types of brain injuries. Learn more about who our patients are.](https://www.cognitivefxusa.com/treatment-outcomes)
[Patient Stories Our patients say it best! Watch our past patients' stories.](https://www.cognitivefxusa.com/patient-stories)
[Other Brain Injuries We have found our approach to concussion treatment also works for other types of brain injuries. Check out our non-concussion patients' improvements with EPIC Treatment.](https://www.cognitivefxusa.com/other-types-of-injuries)
[How We Measure Success Learn more about how we measure the success of EPIC Treatment through our fNCI scan and symptom measurements.](https://www.cognitivefxusa.com/treatment-outcomes)
[Treatment Summary Whitepaper Learn more about the outcomes and studies done on targeted fMRI guided treatment for brain injuries.](https://www.cognitivefxusa.com/hubfs/Treatment%20and%20Research%20Summary/Treatment%20%26%20Research%20Summary%20\(web\).pdf?hsLang=en-us)
- [Blog](https://www.cognitivefxusa.com/blog) 
### The Cognitive FX Head Injury Blog
[Post Concussion Treament Learn more about post-concussion syndrome.](https://www.cognitivefxusa.com/blog/topic/post-concussion-treatment)
[Transcranial Magnetic Stimulation Learn more about TMS for depression, anxiety, and concussion.](https://www.cognitivefxusa.com/blog/topic/transcranial-magnetic-stimulation-tms)
[Long Covid - Viral Infection Treatment Learn more about how we treat viral infections that impact the brain. COVID-19, Lyme, etc.](https://www.cognitivefxusa.com/blog/topic/covid)
[Other Brain Injuries Treated Read about other types of brain injury we treat. Stroke, TIA, Tinnitus, etc.](https://www.cognitivefxusa.com/blog/topic/traumatic-brain-injury)
[Patient Outcomes and Stories Learn more about the specific symptoms and issues our patients have faced.](https://www.cognitivefxusa.com/blog/topic/patient-stories)
[Browse more topics here! Browse through all of the brain injury topics and posts from the Cognitive FX Blog home.](https://www.cognitivefxusa.com/blog)
[**Get Started**](https://cognitivefxusa.typeform.com/depression?typeform-source=www.cognitivefxusa.com)
[Back to Blog](https://www.cognitivefxusa.com/blog)
#### Content
- [Transcranial Magnetic Stimulation (TMS)](https://www.cognitivefxusa.com/blog/fast-acting-depression-treatment-options#transcranial-magnetic-stimulation-tms)
- [Is Your TMS Target Actually in the Right Place?](https://www.cognitivefxusa.com/blog/fast-acting-depression-treatment-options#is-your-tms-target-actually-in-the-right-place)
- [Other Fast-Acting Depression Medications for Treatment-Resistant Depression](https://www.cognitivefxusa.com/blog/fast-acting-depression-treatment-options#other-fast-acting-depression-medications-for-treatment-resistant-depression)
- [Ketamine](https://www.cognitivefxusa.com/blog/fast-acting-depression-treatment-options#ketamine)
- [Esketamine (Brand Name: Spravato)](https://www.cognitivefxusa.com/blog/fast-acting-depression-treatment-options#esketamine-brand-name-spravato)
- [Dextromethorphan-bupropion (Brand Name: Auvelity)](https://www.cognitivefxusa.com/blog/fast-acting-depression-treatment-options#dextromethorphan-bupropion-brand-name-auvelity)
- [Additional Considerations Regarding Traditional Antidepressant Medications](https://www.cognitivefxusa.com/blog/fast-acting-depression-treatment-options#additional-considerations-regarding-traditional-antidepressant-medications)
- [Conclusion](https://www.cognitivefxusa.com/blog/fast-acting-depression-treatment-options#conclusion)
- [Cited Research](https://www.cognitivefxusa.com/blog/fast-acting-depression-treatment-options#cited-research)
1. [Home](https://www.cognitivefxusa.com/)
2. [Blog](https://www.cognitivefxusa.com/blog)
3. Compare the Top Fast-Acting Depression Treatments: Effectiveness, Time Frames & Side Effects
# Compare the Top Fast-Acting Depression Treatments: Effectiveness, Time Frames & Side Effects

Dr. Diane Spangler, Ph.D.
•
Updated on 31 March, 2026
•
Medically Reviewed by
[Dr. Mark Allen](https://www.cognitivefxusa.com/dr-mark-allen-phd)
Play
Fast-Acting Antidepressants: Compare Options & Effectiveness
AI-generated audio
23:35
- [Transcranial Magnetic Stimulation (TMS)](https://www.cognitivefxusa.com/blog/fast-acting-depression-treatment-options#transcranial-magnetic-stimulation-tms)
- [Is Your TMS Target Actually in the Right Place?](https://www.cognitivefxusa.com/blog/fast-acting-depression-treatment-options#is-your-tms-target-actually-in-the-right-place)
- [Other Fast-Acting Depression Medications for Treatment-Resistant Depression](https://www.cognitivefxusa.com/blog/fast-acting-depression-treatment-options#other-fast-acting-depression-medications-for-treatment-resistant-depression)
- [Ketamine](https://www.cognitivefxusa.com/blog/fast-acting-depression-treatment-options#ketamine)
- [Esketamine (Brand Name: Spravato)](https://www.cognitivefxusa.com/blog/fast-acting-depression-treatment-options#esketamine-brand-name-spravato)
- [Dextromethorphan-bupropion (Brand Name: Auvelity)](https://www.cognitivefxusa.com/blog/fast-acting-depression-treatment-options#dextromethorphan-bupropion-brand-name-auvelity)
- [Additional Considerations Regarding Traditional Antidepressant Medications](https://www.cognitivefxusa.com/blog/fast-acting-depression-treatment-options#additional-considerations-regarding-traditional-antidepressant-medications)
- [Conclusion](https://www.cognitivefxusa.com/blog/fast-acting-depression-treatment-options#conclusion)
- [Cited Research](https://www.cognitivefxusa.com/blog/fast-acting-depression-treatment-options#cited-research)
Traditional antidepressant medications involve a trial period of weeks or months before it can be determined whether or not they are working. If a medication doesn’t work — and it’s been [shown](https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10373710/) that **traditional antidepressant medications only work for about one-third of patients** — then the patient must begin another trial with a different drug and go through the process all over again.
Throughout these trials, patients often experience unpleasant side effects that [impact](https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3181894/) their quality of life. And beyond a second failed antidepressant drug, data [suggests](https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10373710/) that less than 2% of patients have success with a third or fourth medication.
Patients need new treatment options that help relieve their symptoms faster, ideally with fewer side effects. In this article, we discuss what’s available at the moment, including:
- [Transcranial magnetic stimulation (TMS)](https://www.cognitivefxusa.com/blog/fast-acting-depression-treatment-options#tms)
- [Ketamine](https://www.cognitivefxusa.com/blog/fast-acting-depression-treatment-options#ketamine)
- [Esketamine](https://www.cognitivefxusa.com/blog/fast-acting-depression-treatment-options#esketamine)
- [Dextromethorphan-bupropion](https://www.cognitivefxusa.com/blog/fast-acting-depression-treatment-options#dextromethorphan-bupropion)
## Transcranial Magnetic Stimulation (TMS)
TMS is a noninvasive, FDA-approved procedure that uses magnetic pulses to restore normal activity levels in a part of the brain called the dorsolateral prefrontal cortex (DLPFC) which is consistently [affected](https://www.nature.com/articles/s41386-021-01101-7) by depression and other mood disorders. During a TMS session, an electromagnetic coil is placed over the patient’s head directly above the DLPFC, and pulses are applied at specific intervals to stimulate nerve cells in that area.
Patients who receive newer forms of TMS can experience relief from their depression in a single week of treatment. TMS also has mild [side effects](https://www.cognitivefxusa.com/blog/side-effects-of-tms-benefits-vs-risks) compared to antidepressant medications which we’ll discuss below.
### Types of TMS
#### Repetitive Transcranial Magnetic Stimulation (the Original Method of TMS)
The original form of TMS was first [used](https://pubmed.ncbi.nlm.nih.gov/8547583/) in the treatment of depression in the mid-90s. This procedure — called **repetitive transcranial magnetic stimulation (rTMS) —** involves [the](https://pubmed.ncbi.nlm.nih.gov/12894031/) application of [repeated](https://pubmed.ncbi.nlm.nih.gov/12894031/) electromagnetic pulses delivered by a magnetic coil placed on the patient’s scalp over the DLPFC area.
Usually, [patients](https://pubmed.ncbi.nlm.nih.gov/31901449/) receive 20-30 TMS sessions, delivered daily over four to six weeks, with each [session](https://www.ncbi.nlm.nih.gov/books/NBK568715/) lasting up to 40 minutes. [Many](https://pubmed.ncbi.nlm.nih.gov/30764649/) patients begin feeling better after just two weeks. [About 50% of patients](https://journals.lww.com/co-psychiatry/fulltext/2019/09000/repetitive_transcranial_magnetic_stimulation.8.aspx) respond well to treatment with over 30% showing complete remission. When combined with psychotherapy, success rates are even more impressive with response and remission rates of ~66% and ~55% respectively.
*Response and remission rates of various monotherapeutic and combinatory antidepressant treatments based on the largest studies and datasets available.* [*\[Source\]*](https://journals.lww.com/co-psychiatry/fulltext/2019/09000/repetitive_transcranial_magnetic_stimulation.8.aspx)
## Is Your TMS Target Actually in the Right Place?
See why the difference between a population average and your exact brain coordinate can determine whether treatment works
Building brain model…
Drag to rotate • Scroll to zoom • Click a marker to explore
×
fMRI-Guided
toggle all
Patient 1Left DLPFC
Patient 2Left DLPFC
Patient 3Left DLPFC
Traditional Targets
toggle all
5cm RuleLeft DLPFC (approx.)
Beam F3 MethodLeft DLPFC (approx.)
Other Targets
toggle all
Right DLPFC EfficacyRight DLPFC
Left Posterior ParietalLeft PPC
Dorsomedial PFCdmPFC
► Visualize Your Approximate Target
X (mm) Y (mm)
Z auto-positioned to nearest cortical surface
Show My Target on Brain
Please enter valid MNI coordinates.
Is Your Target Right?
When It’s Wrong
How CFX Finds Yours
Treatment Outcomes: Standard TMS vs. fMRI-Guided TMS
Treatment-resistant depression populations
100%75%50%25%0%
50%
78%
Response Rate
33%
79%
Remission Rate
Standard TMS (scalp-based targeting) fMRI-Guided TMS (personalized targeting)
► Sources
1 Cole EJ et al. Stanford Neuromodulation Therapy (SNT): A Double-Blind Randomized Controlled Trial. *Am J Psychiatry.* 2022;179(2):132–141. PMID 34711062. (Response 85.7%, Remission 78.6% in fMRI-guided group; ~50% response / ~33% remission for standard rTMS per FDA trial data cited therein.)
2 Shahi N et al. Naturalistic Outcomes with fMRI-Guided and Non-fMRI-Guided Accelerated TMS for Depression. *medRxiv.* 2025. doi:10.1101/2025.09.03.25334813. (Real-world: fMRI-guided 77.5% vs. standard 62% response; 2.3× odds of response with fMRI guidance, n=195.)
3 O’Reardon JP et al. Efficacy and Safety of Transcranial Magnetic Stimulation in the Acute Treatment of Major Depressive Disorder. *Biol Psychiatry.* 2007;62(11):1208–1216. PMID 17573044. (Standard rTMS ~33% remission in pivotal FDA trial.)
#### What Most Clinics Do
- Uses skull measurements or EEG landmarks
- No brain imaging — one coordinate for everyone
- Target can land up to 3cm from your actual circuit
- If it doesn’t work, most clinics have no way to know why
#### What CFX Does
- fMRI maps the specific circuit driving your depression
- Finds your exact DLPFC coordinate — not a population average
- Accounts for how your anatomy differs from everyone else
- If the first treatment doesn’t land perfectly, we can adjust
Standard TMS protocols use a single coordinate derived from population averages. That coordinate may be centimeters away from the specific spot in **your** prefrontal cortex that connects to your depression circuit. When the target is off, the magnetic pulse stimulates tissue that isn’t driving your depression — and treatment fails, not because TMS doesn’t work, but because it didn’t treat *your* brain.
This is likely the most common reason people try TMS and feel like it “didn’t work.” The technology worked. The address was wrong.
Look at the dots on the brain above. The spread between the population-average targets and any custom coordinate you place represents real anatomical variance — variance that determines treatment outcome.
Before your first pulse, Cognitive FX runs a resting-state fMRI scan. That scan maps the connectivity between your prefrontal cortex and the subgenual cingulate — the specific circuit that drives depression. We find the exact voxel in your DLPFC with the strongest connection to that circuit. That voxel becomes your treatment coordinate.
No other clinic in Utah does this. Most TMS providers pick a coordinate from a chart and apply the same protocol to every patient. We treat the brain in front of us.
**Use the panel on the left to enter approximate coordinates and see where your target might fall** — or schedule a consultation and we’ll find your exact location with imaging.
**The data is clear: fMRI-guided targeting produces significantly better outcomes than scalp-based methods.** If you’re considering TMS for depression, the question isn’t whether imaging guidance matters. It’s whether your provider is using it. Talk to us before you start treatment.
[Talk to a CFX Specialist →](https://www.cognitivefxusa.com/treatment-quiz)
#### Accelerated TMS (Reduces Treatment Time to a Single Week)
Showing up to daily sessions for four to six weeks has been impractical for many patients due to work and life commitments. To solve this issue, researchers developed **accelerated TMS**, where patients undergo multiple TMS sessions per day and can complete treatment in a single week.
Accelerated TMS is [as safe](https://pubmed.ncbi.nlm.nih.gov/29153439/) as daily rTMS and potentially more effective. In addition, patients [receiving](https://pubmed.ncbi.nlm.nih.gov/29398915/) multiple sessions each day seem to experience improvements in symptoms faster than those receiving daily sessions, and the effects are still [visible](https://pubmed.ncbi.nlm.nih.gov/32849235/) months after their treatment.
#### Intermittent Theta-Burst Stimulation (a New Method of TMS)
In 2018, the FDA approved a new version of accelerated TMS called [**Intermittent Theta-Burst Stimulation (iTBS)**](https://www.cognitivefxusa.com/blog/theta-burst-stimulation-tms-treatment). Theta waves are the frequencies the hippocampus uses to connect to other brain circuits and are utilized in memory formation, meditation, and certain phases of sleep. Theta burst stimulation uses a different magnetic pulse (in triplets) and delivers the treatment in three minutes (compared to 37 minutes in rTMS).
This method can produce rapid reductions in depression symptoms with many patients [experiencing](https://www.brainstimjrnl.com/article/S1935-861X\(21\)00184-4/fulltext) improvements shortly after starting their treatment. In addition, patients also noticed a decrease in [suicidal](https://www.frontiersin.org/articles/10.3389/fnhum.2016.00480/full) ideation, suggesting that iTBS could be an option to rapidly treat patients at high risk of suicide.
#### fMRI-Guided iTBS (the Newest and Most Effective Method of TMS)
In the standard [rTMS and iTBS protocols](https://www.cognitivefxusa.com/blog/theta-burst-stimulation-itbs-vs-rtms), the location to apply the coil is calculated based on taking manual measurements between the patient’s nose, ears, and top of the head. However, due to variations in head size and shape, or differences in brain organization between patients, [studies](https://pubmed.ncbi.nlm.nih.gov/11457424/) have found this method of coil placement can be imprecise and lead to less consistent outcomes. Even missing the DLPFC by a few millimeters is enough to produce poorer results.
To overcome this limitation, researchers began using functional MRI and neuronavigation devices to determine exactly where the DLPFC is located in the depressed patient’s brain. This method, developed by a team from Stanford University, is known as the SAINT™ protocol. SAINT stands for Stanford Intelligent Accelerated Neuromodulation Therapy. The FDA [approved](https://www.accessdata.fda.gov/cdrh_docs/pdf22/K220177.pdf) SAINT depression treatment in September 2022, and it is now regarded as the “gold standard” treatment for treatment-resistant depression.

*A comparison of remission rates for rTMS/iTBS, electroconvulsive therapy (ECT), and SAINT-iTBS.*
The SAINT™ protocol involves 10 sessions per day over five days for 50 sessions total. In a double-blind randomized clinical trial, [**about 85.7%**](https://ajp.psychiatryonline.org/doi/10.1176/appi.ajp.2021.20101429?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%20%200pubmed) **of patients responded to the SAINT-iTBS treatment** (meaning they met prespecified criteria for reduced depressive symptoms) **and around 78.6% met the remission criterion.** All the individuals in the study had treatment-resistant depression and had failed at least two other depression treatments. **One month after treatment, 60% were still in remission**.
The speed with which SAINT-iTBS can achieve high response and remission rates makes it one of the best rapid-acting treatments for depression available today. However, there is limited data on the durability of these outcomes and how well they hold up over time. Some patients see lasting remission or symptom reduction, while others need follow-up treatments to maintain the effectiveness. Studies show that TMS maintenance sessions can be extremely helpful, sometimes allowing patients to stay [symptom-free](https://pubmed.ncbi.nlm.nih.gov/28951141/) for up to eight years.
In addition, combining TMS with cognitive behavioral therapy (CBT), as we do at our clinic, is likely to produce the best long-term outcomes for patients. While there are no studies yet combining iTBS and CBT, one [study](https://www.brainstimjrnl.com/article/S1935-861X\(17\)30960-9/fulltext) found that combining rTMS and CBT nearly doubled remission rates for patients.
### Side Effects and Contraindications
TMS is a safe procedure with only [mild and short-lived side effects](https://www.cognitivefxusa.com/blog/side-effects-of-tms-benefits-vs-risks), such as headaches, neck pain, or a tingling sensation in the scalp. These symptoms usually go away after a few sessions. The most serious complication is a seizure, but the risk is extremely low — less than 0.001% per session. Even if a seizure does occur, patients recover quickly and fully without any long-term effects.
TMS cannot be used if you have certain metallic implants or objects in your brain near where the coil is placed. This includes devices like cochlear implants, Internal Pulse Generators, medication pumps, aneurysm clips or coils, stents, or bullet fragments. However, braces and dental fillings are safe and won't interfere with treatment.
Some medications can increase the risk of seizures and might prevent you from having TMS. If you are on medication, it’s important to talk to your healthcare professional before starting TMS. For patients taking drugs with a high risk of seizures, TMS should be used with caution.
### Receiving fMRI-Guided TMS at Cognitive FX
Our clinic in Provo, Utah, provides an alternative to SAINT™ TMS that offers the same precision of personalized treatment targeting, combined with FDA-approved theta burst stimulation at a significantly lower cost. This approach delivers the same core elements that make SAINT so revolutionary.
The only difference between our treatment and SAINT™ (a trademark licensed to Stanford Medical) is our targeting method. Our target locations are determined by fMRI and our prescribing neuroscientist and physician, rather than their proprietary software.
# Accelerated fMRI - TMS vs. Magnus SAINT™ TMS
| | Accelerated fMRI - TMS | Magnus SAINT™ TMS |
|---|---|---|
| FDA-Approved iTBS | ✔ | ✔ |
| FDA-Approved Neuronavigators | ✔ | ✔ |
| FDA-Approved Figure 8 Coils | ✔ | ✔ |
| Number of Treatment Days | 5 | 5 |
| Treatments per Day | 10 | 10 |
| Total Treatments | 50 | 50 |
| Number of TMS Pulses | Approx. 90,000 | 90,000 |
| Resting motor threshold pulse intensity | 90–120% | 90–120% |
| FDA-Approved Personalized DLPFC Targeting | ✘ | ✔ |
| Personalized DLPFC Targeting Assists Doctor in Target Location | ✔ | ✘ |
| Personalized E Field Coil orientation | ✔ | ✘ |
| Cost | \$9,000 to \$12,000 | \$30,000+ |
This accelerated protocol of iTBS is:
- **Safe:** Widely tolerated and associated with mild, short-lasting side effects.
- **Precise:** fMRI ensures that the treatment target area is precisely located for each patient, accounting for variations in head size and shape. Neuronavigation ensures the magnetic coil is placed over that exact spot for every treatment session.
- **Fast:** Treatment courses are reduced to a single week, making it easier to complete alongside life and work commitments (compared to 4 to 6 weeks of standard TMS and accelerated TMS protocols).
- **Effective:** Precision coil placement combined with theta burst stimulation produces the [best TMS treatment results to date](https://www.cognitivefxusa.com/blog/most-effective-depression-treatments).
To improve patient outcomes, we also include cognitive behavioral therapy (CBT) as a part of our treatment. When combined with the traditional method of TMS (rTMS), CBT [improved response and remission rates](https://journals.lww.com/co-psychiatry/fulltext/2019/09000/repetitive_transcranial_magnetic_stimulation.8.aspx) by ~8% and ~19%, respectively. Additionally, CBT is likely to produce sustained improvement over time once treatment has concluded.
Our brain stimulation treatment is ideal for most patients with treatment-resistant depression. However, we do not treat patients under the age of 18 or over 65. Additionally, as a safety measure, we do not treat patients who have a history of seizures or who are currently actively suicidal and in need of crisis care.
[***Click here***](https://www.cognitivefxusa.com/tms-new-patient-paperwork) *to learn more about receiving accelerated fMRI TMS therapy at Cognitive FX.*
## Other Fast-Acting Depression Medications for Treatment-Resistant Depression
Recent efforts to develop new pharmaceuticals for treating depression have primarily focused on increasing the levels of serotonin in the brain. However, the idea that depression is caused by low serotonin levels is still just a hypothesis.
Over the past three decades, [compelling](https://pubmed.ncbi.nlm.nih.gov/17574216/) evidence has indicated that the neurotransmitter glutamate also plays a role in depressive symptoms. This research has enhanced our understanding of the brain mechanisms behind depression and has led to the development of new fast-acting antidepressants, such as ketamine, esketamine, and dextromethorphan-bupropion.
These antidepressants bind to N-methyl-D-aspartate (NMDA) receptors in the brain and block the activity of glutamate, an excess of which is thought to [contribute](https://pubmed.ncbi.nlm.nih.gov/27096778/) to depression. However, glutamate is also an important neurotransmitter involved in memory and learning and is important for overall healthy brain function. By inhibiting it, some patients may [experience](https://www.sciencedirect.com/science/article/abs/pii/S0278584622000677) cognitive impairments, a trade-off that patients should consider before starting any of these treatments. (TMS, in contrast, does not have this downside. Brain stimulation can *improve* the function of glutamate and other neurotransmitters and promote better brain function.)
## Ketamine
Ketamine was approved by the FDA in 1970 to be used as an anesthetic. In 2000, a [clinical trial](https://www.sciencedirect.com/science/article/pii/S0006322399002309?via%3Dihub) showed that ketamine could be used to improve the mood of patients living with depression. Since then, multiple clinical trials have shown that ketamine is extremely fast-acting compared with traditional antidepressants and can [relieve](https://pubmed.ncbi.nlm.nih.gov/33065824/) depressive symptoms, including [suicidal](https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5880701/) ideation, for a period that can last days or weeks. Around [60%](https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3992936/) of patients experienced the benefits of ketamine up to three days after a single treatment and about 40% of these patients still had not relapsed a month later. However, after six [months](https://www.psychiatrist.com/jcp/clinical-outcomes-intravenous-ketamine-for-depression-va-health-system/) and multiple ketamine treatments, only 26% of patients were still responding and only 15% were symptom-free and in remission.
In chemical terms, ketamine is a chiral molecule, meaning it has two chemical forms that are mirror images of each other: R-Ketamine and S-Ketamine. Racemic ketamine is a mixture of both R-Ketamine and S-Ketamine in equal parts and is the most commonly used form of ketamine in clinical settings.
Ketamine is administered to patients intravenously. During this procedure, patients are closely monitored by a healthcare professional because ketamine is a dissociative drug, which means patients can feel disconnected from reality and engage in dangerous and life-threatening behaviors. In addition, patients may also experience severe side effects, including:
- Dissociation
- Intoxication
- Sedation
- High blood pressure
- Dizziness
- Headache
- Blurred vision
- Anxiety
- Nausea and vomiting
A typical treatment plan includes four to six sessions over two to three weeks. Some patients need booster sessions, typically once a month or once every three months, depending on the patient. To boost the effects of ketamine, it is recommended to combine it with a form of psychotherapy, such as cognitive behavioral therapy (CBT).
The surge in demand for this drug has paved the way for a cottage industry of clinics offering ketamine treatments. Some companies make sweeping claims that they’re able to treat dozens of conditions, including depression, anxiety, chronic pain, PTSD, bipolar disorder, and migraines. Such claims are currently not backed by scientific studies. As the industry is unregulated, the quality of care received at these clinics [can be highly variable.](https://www.statnews.com/2018/09/24/ketamine-clinics-severe-depression-treatment/) Many clinics are not run by doctors of psychiatry and are simply pain management clinics that have added ketamine to their list of treatments or are spas with staff not trained in mental health treatment. In addition, it can be expensive. Typically, treatments cost between \$400 to \$1,000 per session, which can add up to thousands for the full treatment. If you’re considering this option, our advice is to discuss it with your family doctor before committing to any clinic.
## Esketamine (Brand Name: Spravato)
Ketamine shows some promise in treating treatment-resistant depression, but the IV administration is time-consuming. To overcome these issues, researchers developed a new antidepressant using only the S-ketamine fraction, aptly named Esketamine. In 2019, the FDA approved this product as a nasal spray for easy application, sold under the brand name Spravato.
Clinical [studies](https://pubmed.ncbi.nlm.nih.gov/31109201/) have shown that S-ketamine has fast antidepressant effects, with some patients reporting a reduction in symptoms [within](https://psychiatryonline.org/doi/10.1176/appi.ajp.2019.19020172?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%20%200pubmed) hours of administration. This is in contrast to traditional antidepressant medications that can take weeks or months to take effect. This makes it particularly beneficial for patients who have not responded to other treatments or are in urgent need of treatment due to severe suicidal tendencies. After an eight-week treatment, [about](https://www.nejm.org/doi/10.1056/NEJMoa2304145) one third of patients had achieved remission and, of these, about one third had not relapsed more than eight months later.
Spravato comes with specific guidelines for administration due to potential side effects such as nausea, headaches, dizziness, disorientation, and dissociation immediately after use. It must be administered at certified treatment centers under the supervision of a mental health care professional. Ideally, esketamine should be used in conjunction with a conventional antidepressant medication. The aim is to use esketamine for fast relief from depression symptoms until the other medication takes effect.
In most cases, patients receive esketamine twice a week for the first month, and then if patients improve, they continue to receive the drug at a lower frequency for a few weeks or months. Typically, this means treatments start as weekly, then drop to every two weeks, then monthly, etc.
### Arketamine
Researchers have also tested the R-ketamine fraction — called arketamine — to treat major depression and other mental health conditions, but this drug has not received approval from the FDA yet.
[Preliminary](https://pubmed.ncbi.nlm.nih.gov/35977629/) results are encouraging, with antidepressant effects faster and longer than ketamine and fewer side effects, especially in terms of dissociation and hallucinations. Clinical trials are currently underway in the US and other locations around the world.
In addition to its antidepressant-like effects, arketamine may help treat patients with various neurological disorders, such as Parkinson's disease and multiple sclerosis. Moreover, [arketamine](https://linkinghub.elsevier.com/retrieve/pii/S0028390822002301) has anti-inflammatory, bronchodilating, and neuroprotective effects, which means it could be a new [drug](https://www.nature.com/articles/s41380-021-01121-1) for patients with neurological disorders and inflammatory diseases.
## Dextromethorphan-bupropion (Brand Name: Auvelity)
A new fast-acting medication called Auvelity was just approved by the US Food and Drug Administration to treat patients with major depressive disorder (MDD). Auvelity is a combination of two already existing drugs: dextromethorphan and bupropion.
Dextromethorphan is commonly used in cough syrups to provide temporary relief from cough. Recent [research](https://www.tandfonline.com/doi/abs/10.1080/14728214.2021.1898588) showed it can also be used to alleviate depressive symptoms, but it’s metabolized very quickly in the body. Bupropion is an existing antidepressant medication, which also slows down the metabolism of dextromethorphan in the body. Staying in the body longer means the levels of drugs are more stable and can potentially help patients more.
A phase three [clinical trial](https://www.psychiatrist.com/jcp/efficacy-safety-of-axs-05-dextromethorphan-bupropion-mdd/) confirmed that Auvelity can improve symptoms of depression and a few patients started experiencing the benefits after just one week. After six weeks, over 50% of the patients responded to the treatment and were feeling better and 40% were in remission which is a slightly higher remission rate than for other types of antidepressant medications. Crucially, this [combination](https://psychiatryonline.org/doi/full/10.1176/appi.ajp.21080800) works significantly better than bupropion alone. After six weeks, only about 40% of patients responded to bupropion in isolation, and less than 20% achieved remission.
Auvelity doesn’t have the same safety restrictions as ketamine, making it a much safer alternative. Typically, it has similar [side effects](https://psychiatryonline.org/doi/full/10.1176/appi.ajp.21080800) and warnings compared to existing antidepressant medications, including dizziness, nausea, dry mouth, decreased appetite, and anxiety.
There is a risk that Auvelity may increase suicidal thoughts and actions in young adults, adolescents, and children. For this reason, it’s essential to pay close attention to sudden changes in mood, behavior, thoughts, feelings, or suicidal thoughts when taking this drug.
Additionally, Auvelity should not be taken by patients with a history of seizures, or eating disorders, or those taking other antidepressants like monoamine oxidase inhibitors, benzodiazepines, barbiturates, or anti-seizure medicines.
## Additional Considerations Regarding Traditional Antidepressant Medications
As described earlier, most antidepressants take weeks or months for patients to begin experiencing the benefits (if they experience benefits at all). However, there is some [evidence](https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2211759/) that a few antidepressants work faster in some patients but there are no reliable ways to determine which patients will respond faster. These include, for example, some selective serotonin reuptake inhibitors (SSRIs), serotonin-norepinephrine reuptake inhibitors (SNRIs), and tricyclic antidepressants (TCAs).
SSRIs and SNRIs aim to increase the levels of serotonin and norepinephrine in the brain. They’re often the first option primary care doctors prescribe because they generally cause fewer side effects. Patients may experience better quality of sleep, higher levels of energy, and increased appetite within the first 1-2 weeks after starting treatment. Improvement in these physical symptoms can be an important early signal that the medication is working. In most cases, severe symptoms may still need up to 6-8 weeks to fully improve.
Some common examples of these drugs include:
- **SSRIs**
- Citalopram (Celesta)
- Fluoxetine (Prozac)
- Sertraline (Zoloft)
- **SNRIs**
- Venlafaxine (Effexor)
- Desvenlafaxine (Pristiq)
- Duloxetine (Cymbalta)
Similarly to SNRIs, tricyclic antidepressants also aim to increase the levels of serotonin and norepinephrine, but they tend to cause more side effects. They’re typically only prescribed for patients who have tried other antidepressants without improvement. One example of a fast-acting tricyclic antidepressant is called desipramine, and [more](https://www.nature.com/articles/1300341.pdf) than 50% of patients experience significant improvements during the first week of treatment.
However, it is important to note that response times to antidepressant medications vary greatly from patient to patient, and it is crucial to consult with a healthcare professional to determine the most appropriate treatment approach for an individual’s specific needs.
## Conclusion
The treatment landscape for depression is evolving, with new options providing faster relief and potentially fewer side effects compared to traditional antidepressant medications. Traditional medications often involve a lengthy trial period and can come with unpleasant side effects, with only about one-third of patients having reliable reductions in depression symptoms.
Among the newer treatments, TMS stands out for its noninvasiveness and rapid effectiveness. Accelerated fMRI theta burst stimulation, in particular, offers a significant advancement by using fMRI and neuronavigation for precise coil placement, leading to high response and remission rates within a single week of treatment. This method, available at our clinic, is among the most effective fast-acting treatments for depression, with the added advantage of not impairing cognitive functions.
Other fast-acting treatments like ketamine, esketamine, and dextromethorphan-bupropion provide rapid symptom relief by targeting neurotransmitters such as glutamate. However, these treatments can come with side effects that patients should consider carefully, and the effects of these treatments are often not long-lasting.
Ultimately, the combination of fMRI TMS with cognitive behavioral therapy (CBT) offers a promising solution for many patients with treatment-resistant depression. This integrated approach not only provides rapid symptom relief but also promotes sustained improvement in brain function and overall mental health.
*If you are interested in receiving accelerated fMRI TMS therapy at Cognitive FX,* [*click here to learn more*](https://www.cognitivefxusa.com/tms-new-patient-paperwork) *and see if you’re a good fit for treatment.*
## Cited Research
- [A reanalysis of the STAR\*D study’s patient-level data with fidelity to the original research protocol](https://pmc.ncbi.nlm.nih.gov/articles/PMC10373710/)
- [Repetitive transcranial magnetic stimulation treatment for depressive disorders](https://journals.lww.com/co-psychiatry/fulltext/2019/09000/repetitive_transcranial_magnetic_stimulation.8.aspx)
- [Stanford Neuromodulation Therapy (SNT): A Double-Blind Randomized Controlled Trial](https://psychiatryonline.org/doi/10.1176/appi.ajp.2021.20101429?url_ver=Z39.88-2003&rfr_id=ori%3Arid%3Acrossref.org&rfr_dat=cr_pub++0pubmed)
- [Antidepressant effects of ketamine in depressed patients](https://www.sciencedirect.com/science/article/abs/pii/S0006322399002309?via%3Dihub)
- [Efficacy and Safety of Flexibly Dosed Esketamine Nasal Spray Combined With a Newly Initiated Oral Antidepressant in Treatment-Resistant Depression: A Randomized Double-Blind Active-Controlled Study](https://psychiatryonline.org/doi/10.1176/appi.ajp.2019.19020172)
***

### About the author
[Dr. Diane Spangler, Ph.D.](https://www.cognitivefxusa.com/blog/author/dr-diane-spangler-phd)
Dr. Spangler is a Clinical Psychologist with over 20 years of experience working in both clinical and academic settings. She earned her doctorate degree in Clinical Psychology at the University of Oregon followed by a Postdoctoral Research Fellowship in the Department of Psychiatry at the Stanford University School of Medicine. Dr. Spangler served as a Professor of Psychology at Brigham Young University for 15 years where she directed training in Cognitive Behavioral Therapy for the Clinical Psychology Doctoral Program, and conducted research on the etiology and treatment of depressive, anxiety, and eating disorders. She also served as a Visiting Professor in the Department of Psychiatry Cognitive Therapy Centre at Oxford University in England. Dr Spangler has authored over 60 publications and has lectured worldwide. She has received numerous awards for her collective work from the National Institute of Mental Health, the American Psychological Association, the International Association for Cognitive Psychotherapy, the Association for Behavioral and Cognitive Therapies, the Beck Institute, and the National Association of Professional Women.
## Related Posts
Previous

### TMS vs. tDCS for Depression: Which Is Better?

[Dr. Mark Allen, Ph.D.](https://www.cognitivefxusa.com/blog/author/dr-diane-spangler-phd)
For many people living with major depression, antidepressant medications either [don’t work](https://www.cognitivefxusa.com/blog/why-arent-my-antidepressant-medications-working) or only get them part of the way to recovery. Symptoms may ease for a while, but then return, or never fully...
[Read the full article](https://www.cognitivefxusa.com/blog/tms-vs-tdcs)
### TMS Therapy vs. Neurofeedback: Which Is Better for Depression?

[Dr. Mark Allen, Ph.D.](https://www.cognitivefxusa.com/blog/author/dr-diane-spangler-phd)
Transcranial magnetic stimulation (TMS) and neurofeedback are gaining popularity as non-invasive, medication-free options for treating depression—especially for people who haven’t found relief from [...](https://www.cognitivefxusa.com/blog/why-arent-my-antidepressant-medications-working)
[Read the full article](https://www.cognitivefxusa.com/blog/tms-therapy-vs-neurofeedback-for-depression)

### How Long Has TMS Been Around?

[Dr. Mark Allen, Ph.D.](https://www.cognitivefxusa.com/blog/author/dr-diane-spangler-phd)
While many people are learning about Transcranial Magnetic Stimulation (TMS) for the first time, this [brain stimulation method](https://www.cognitivefxusa.com/blog/brain-stimulation-depression-treatment) has been helping patients for nearly 40 years. Originally developed as...
[Read the full article](https://www.cognitivefxusa.com/blog/how-long-has-tms-been-around)

### TMS vs VNS for Depression: Which Treatment Is Better?

[Dr. Mark Allen, Ph.D.](https://www.cognitivefxusa.com/blog/author/dr-diane-spangler-phd)
Both **Transcranial Magnetic Stimulation (TMS)** and **Vagus Nerve Stimulation (VNS)** are FDA-approved neuromodulation treatments for depression. At first glance, they may seem similar—both use electricity...
[Read the full article](https://www.cognitivefxusa.com/blog/tms-vs-vns-for-depression)

### Side Effects of TMS: Do the Benefits Outweigh the Risks?

[Dr. Mark Allen, Ph.D.](https://www.cognitivefxusa.com/blog/author/dr-diane-spangler-phd)
If you’re considering transcranial magnetic stimulation (TMS) therapy, you may be concerned about its side effects and whether the benefits outweigh any risks.
[Read the full article](https://www.cognitivefxusa.com/blog/side-effects-of-tms-benefits-vs-risks)

### Brain Stimulation Depression Treatment: Types & Effectiveness

[Dr. Mark Allen, Ph.D.](https://www.cognitivefxusa.com/blog/author/dr-diane-spangler-phd)
While antidepressant medications remain the most common first-line treatment for depression, [research shows](https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10373710/) they only work for about one-third of patients and often come with unpleasant side effects...
[Read the full article](https://www.cognitivefxusa.com/blog/brain-stimulation-depression-treatment)
Next
[](https://www.cognitivefxusa.com/)
Comprehensive Traumatic Brain Injury Treatment
280 W River Park Drive Suite 110 Provo, UT 84604
#### Quick Links
- [Blog](https://www.cognitivefxusa.com/blog)
- [Sign-Up for Free Consultation](https://www.cognitivefxusa.com/start-here-paperwork-old)
#### Support
- [Contact Us](https://www.cognitivefxusa.com/contactus)
- [Patient Results](https://www.cognitivefxusa.com/treatment-outcomes)
- [Privacy Policy](https://www.cognitivefxusa.com/privacypolicy)
- [Terms & Conditions](https://www.cognitivefxusa.com/terms-and-conditions)
#### Solutions
- [Good Fit Quiz](https://www.cognitivefxusa.com/start-here-paperwork-old)
- [EPIC Treatment](https://www.cognitivefxusa.com/treatment)
- [Post-Concussion Syndrome Information](https://www.cognitivefxusa.com/blog/post-concussion-syndrome-and-post-concussion-symptoms-pcs)
- [fNCI Brain Scan](https://www.cognitivefxusa.com/about-fnci)
- [Online Course](https://cognitivefx.thinkific.com/courses/headaches)
#### Company
- [About](https://www.cognitivefxusa.com/research-history)
- [Press & Media](https://www.cognitivefxusa.com/media)
- [Our Team](https://www.cognitivefxusa.com/our-team)
### Sign Up For Our Newsletter
Copyright © Cognitive FX 2024. All Rights Reserved. \| [Privacy Policy](https://www.cognitivefxusa.com/blog/fast-acting-depression-treatment-options) |
| Readable Markdown | ## Compare the Top Fast-Acting Depression Treatments: Effectiveness, Time Frames & Side Effects

•
Updated on 31 March, 2026
•
Traditional antidepressant medications involve a trial period of weeks or months before it can be determined whether or not they are working. If a medication doesn’t work — and it’s been [shown](https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10373710/) that **traditional antidepressant medications only work for about one-third of patients** — then the patient must begin another trial with a different drug and go through the process all over again. Throughout these trials, patients often experience unpleasant side effects that [impact](https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3181894/) their quality of life. And beyond a second failed antidepressant drug, data [suggests](https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10373710/) that less than 2% of patients have success with a third or fourth medication. Patients need new treatment options that help relieve their symptoms faster, ideally with fewer side effects. In this article, we discuss what’s available at the moment, including: [Transcranial magnetic stimulation (TMS)](https://www.cognitivefxusa.com/blog/fast-acting-depression-treatment-options#tms) [Ketamine](https://www.cognitivefxusa.com/blog/fast-acting-depression-treatment-options#ketamine) [Esketamine](https://www.cognitivefxusa.com/blog/fast-acting-depression-treatment-options#esketamine) [Dextromethorphan-bupropion](https://www.cognitivefxusa.com/blog/fast-acting-depression-treatment-options#dextromethorphan-bupropion) Transcranial Magnetic Stimulation (TMS) TMS is a noninvasive, FDA-approved procedure that uses magnetic pulses to restore normal activity levels in a part of the brain called the dorsolateral prefrontal cortex (DLPFC) which is consistently [affected](https://www.nature.com/articles/s41386-021-01101-7) by depression and other mood disorders. During a TMS session, an electromagnetic coil is placed over the patient’s head directly above the DLPFC, and pulses are applied at specific intervals to stimulate nerve cells in that area. Patients who receive newer forms of TMS can experience relief from their depression in a single week of treatment. TMS also has mild [side effects](https://www.cognitivefxusa.com/blog/side-effects-of-tms-benefits-vs-risks) compared to antidepressant medications which we’ll discuss below. Types of TMS Repetitive Transcranial Magnetic Stimulation (the Original Method of TMS) The original form of TMS was first [used](https://pubmed.ncbi.nlm.nih.gov/8547583/) in the treatment of depression in the mid-90s. This procedure — called **repetitive transcranial magnetic stimulation (rTMS) —** involves [the](https://pubmed.ncbi.nlm.nih.gov/12894031/) application of [repeated](https://pubmed.ncbi.nlm.nih.gov/12894031/) electromagnetic pulses delivered by a magnetic coil placed on the patient’s scalp over the DLPFC area. Usually, [patients](https://pubmed.ncbi.nlm.nih.gov/31901449/) receive 20-30 TMS sessions, delivered daily over four to six weeks, with each [session](https://www.ncbi.nlm.nih.gov/books/NBK568715/) lasting up to 40 minutes. [Many](https://pubmed.ncbi.nlm.nih.gov/30764649/) patients begin feeling better after just two weeks. [About 50% of patients](https://journals.lww.com/co-psychiatry/fulltext/2019/09000/repetitive_transcranial_magnetic_stimulation.8.aspx) respond well to treatment with over 30% showing complete remission. When combined with psychotherapy, success rates are even more impressive with response and remission rates of ~66% and ~55% respectively.  *Response and remission rates of various monotherapeutic and combinatory antidepressant treatments based on the largest studies and datasets available.* [*\[Source\]*](https://journals.lww.com/co-psychiatry/fulltext/2019/09000/repetitive_transcranial_magnetic_stimulation.8.aspx) Accelerated TMS (Reduces Treatment Time to a Single Week) Showing up to daily sessions for four to six weeks has been impractical for many patients due to work and life commitments. To solve this issue, researchers developed **accelerated TMS**, where patients undergo multiple TMS sessions per day and can complete treatment in a single week. Accelerated TMS is [as safe](https://pubmed.ncbi.nlm.nih.gov/29153439/) as daily rTMS and potentially more effective. In addition, patients [receiving](https://pubmed.ncbi.nlm.nih.gov/29398915/) multiple sessions each day seem to experience improvements in symptoms faster than those receiving daily sessions, and the effects are still [visible](https://pubmed.ncbi.nlm.nih.gov/32849235/) months after their treatment. Intermittent Theta-Burst Stimulation (a New Method of TMS) In 2018, the FDA approved a new version of accelerated TMS called [**Intermittent Theta-Burst Stimulation (iTBS)**](https://www.cognitivefxusa.com/blog/theta-burst-stimulation-tms-treatment). Theta waves are the frequencies the hippocampus uses to connect to other brain circuits and are utilized in memory formation, meditation, and certain phases of sleep. Theta burst stimulation uses a different magnetic pulse (in triplets) and delivers the treatment in three minutes (compared to 37 minutes in rTMS). This method can produce rapid reductions in depression symptoms with many patients [experiencing](https://www.brainstimjrnl.com/article/S1935-861X\(21\)00184-4/fulltext) improvements shortly after starting their treatment. In addition, patients also noticed a decrease in [suicidal](https://www.frontiersin.org/articles/10.3389/fnhum.2016.00480/full) ideation, suggesting that iTBS could be an option to rapidly treat patients at high risk of suicide. fMRI-Guided iTBS (the Newest and Most Effective Method of TMS) In the standard [rTMS and iTBS protocols](https://www.cognitivefxusa.com/blog/theta-burst-stimulation-itbs-vs-rtms), the location to apply the coil is calculated based on taking manual measurements between the patient’s nose, ears, and top of the head. However, due to variations in head size and shape, or differences in brain organization between patients, [studies](https://pubmed.ncbi.nlm.nih.gov/11457424/) have found this method of coil placement can be imprecise and lead to less consistent outcomes. Even missing the DLPFC by a few millimeters is enough to produce poorer results. To overcome this limitation, researchers began using functional MRI and neuronavigation devices to determine exactly where the DLPFC is located in the depressed patient’s brain. This method, developed by a team from Stanford University, is known as the SAINT™ protocol. SAINT stands for Stanford Intelligent Accelerated Neuromodulation Therapy. The FDA [approved](https://www.accessdata.fda.gov/cdrh_docs/pdf22/K220177.pdf) SAINT depression treatment in September 2022, and it is now regarded as the “gold standard” treatment for treatment-resistant depression.  *A comparison of remission rates for rTMS/iTBS, electroconvulsive therapy (ECT), and SAINT-iTBS.* The SAINT™ protocol involves 10 sessions per day over five days for 50 sessions total. In a double-blind randomized clinical trial, [**about 85.7%**](https://ajp.psychiatryonline.org/doi/10.1176/appi.ajp.2021.20101429?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%20%200pubmed) **of patients responded to the SAINT-iTBS treatment** (meaning they met prespecified criteria for reduced depressive symptoms) **and around 78.6% met the remission criterion.** All the individuals in the study had treatment-resistant depression and had failed at least two other depression treatments. **One month after treatment, 60% were still in remission**. The speed with which SAINT-iTBS can achieve high response and remission rates makes it one of the best rapid-acting treatments for depression available today. However, there is limited data on the durability of these outcomes and how well they hold up over time. Some patients see lasting remission or symptom reduction, while others need follow-up treatments to maintain the effectiveness. Studies show that TMS maintenance sessions can be extremely helpful, sometimes allowing patients to stay [symptom-free](https://pubmed.ncbi.nlm.nih.gov/28951141/) for up to eight years. In addition, combining TMS with cognitive behavioral therapy (CBT), as we do at our clinic, is likely to produce the best long-term outcomes for patients. While there are no studies yet combining iTBS and CBT, one [study](https://www.brainstimjrnl.com/article/S1935-861X\(17\)30960-9/fulltext) found that combining rTMS and CBT nearly doubled remission rates for patients. Side Effects and Contraindications TMS is a safe procedure with only [mild and short-lived side effects](https://www.cognitivefxusa.com/blog/side-effects-of-tms-benefits-vs-risks), such as headaches, neck pain, or a tingling sensation in the scalp. These symptoms usually go away after a few sessions. The most serious complication is a seizure, but the risk is extremely low — less than 0.001% per session. Even if a seizure does occur, patients recover quickly and fully without any long-term effects. TMS cannot be used if you have certain metallic implants or objects in your brain near where the coil is placed. This includes devices like cochlear implants, Internal Pulse Generators, medication pumps, aneurysm clips or coils, stents, or bullet fragments. However, braces and dental fillings are safe and won't interfere with treatment. Some medications can increase the risk of seizures and might prevent you from having TMS. If you are on medication, it’s important to talk to your healthcare professional before starting TMS. For patients taking drugs with a high risk of seizures, TMS should be used with caution. Receiving fMRI-Guided TMS at Cognitive FX Our clinic in Provo, Utah, provides an alternative to SAINT™ TMS that offers the same precision of personalized treatment targeting, combined with FDA-approved theta burst stimulation at a significantly lower cost. This approach delivers the same core elements that make SAINT so revolutionary. The only difference between our treatment and SAINT™ (a trademark licensed to Stanford Medical) is our targeting method. Our target locations are determined by fMRI and our prescribing neuroscientist and physician, rather than their proprietary software. Accelerated fMRI - TMS vs. Magnus SAINT™ TMS Accelerated fMRI - TMS Magnus SAINT™ TMS FDA-Approved iTBS ✔ ✔ FDA-Approved Neuronavigators ✔ ✔ FDA-Approved Figure 8 Coils ✔ ✔ Number of Treatment Days 5 5 Treatments per Day 10 10 Total Treatments 50 50 Number of TMS Pulses Approx. 90,000 90,000 Resting motor threshold pulse intensity 90–120% 90–120% FDA-Approved Personalized DLPFC Targeting ✘ ✔ Personalized DLPFC Targeting Assists Doctor in Target Location ✔ ✘ Personalized E Field Coil orientation ✔ ✘ Cost \$9,000 to \$12,000 \$30,000+ This accelerated protocol of iTBS is: **Safe:** Widely tolerated and associated with mild, short-lasting side effects. **Precise:** fMRI ensures that the treatment target area is precisely located for each patient, accounting for variations in head size and shape. Neuronavigation ensures the magnetic coil is placed over that exact spot for every treatment session. **Fast:** Treatment courses are reduced to a single week, making it easier to complete alongside life and work commitments (compared to 4 to 6 weeks of standard TMS and accelerated TMS protocols). **Effective:** Precision coil placement combined with theta burst stimulation produces the [best TMS treatment results to date](https://www.cognitivefxusa.com/blog/most-effective-depression-treatments). To improve patient outcomes, we also include cognitive behavioral therapy (CBT) as a part of our treatment. When combined with the traditional method of TMS (rTMS), CBT [improved response and remission rates](https://journals.lww.com/co-psychiatry/fulltext/2019/09000/repetitive_transcranial_magnetic_stimulation.8.aspx) by ~8% and ~19%, respectively. Additionally, CBT is likely to produce sustained improvement over time once treatment has concluded. Our brain stimulation treatment is ideal for most patients with treatment-resistant depression. However, we do not treat patients under the age of 18 or over 65. Additionally, as a safety measure, we do not treat patients who have a history of seizures or who are currently actively suicidal and in need of crisis care. [***Click here***](https://www.cognitivefxusa.com/tms-new-patient-paperwork) *to learn more about receiving accelerated fMRI TMS therapy at Cognitive FX.* Other Fast-Acting Depression Medications for Treatment-Resistant Depression Recent efforts to develop new pharmaceuticals for treating depression have primarily focused on increasing the levels of serotonin in the brain. However, the idea that depression is caused by low serotonin levels is still just a hypothesis. Over the past three decades, [compelling](https://pubmed.ncbi.nlm.nih.gov/17574216/) evidence has indicated that the neurotransmitter glutamate also plays a role in depressive symptoms. This research has enhanced our understanding of the brain mechanisms behind depression and has led to the development of new fast-acting antidepressants, such as ketamine, esketamine, and dextromethorphan-bupropion. These antidepressants bind to N-methyl-D-aspartate (NMDA) receptors in the brain and block the activity of glutamate, an excess of which is thought to [contribute](https://pubmed.ncbi.nlm.nih.gov/27096778/) to depression. However, glutamate is also an important neurotransmitter involved in memory and learning and is important for overall healthy brain function. By inhibiting it, some patients may [experience](https://www.sciencedirect.com/science/article/abs/pii/S0278584622000677) cognitive impairments, a trade-off that patients should consider before starting any of these treatments. (TMS, in contrast, does not have this downside. Brain stimulation can *improve* the function of glutamate and other neurotransmitters and promote better brain function.) Ketamine Ketamine was approved by the FDA in 1970 to be used as an anesthetic. In 2000, a [clinical trial](https://www.sciencedirect.com/science/article/pii/S0006322399002309?via%3Dihub) showed that ketamine could be used to improve the mood of patients living with depression. Since then, multiple clinical trials have shown that ketamine is extremely fast-acting compared with traditional antidepressants and can [relieve](https://pubmed.ncbi.nlm.nih.gov/33065824/) depressive symptoms, including [suicidal](https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5880701/) ideation, for a period that can last days or weeks. Around [60%](https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3992936/) of patients experienced the benefits of ketamine up to three days after a single treatment and about 40% of these patients still had not relapsed a month later. However, after six [months](https://www.psychiatrist.com/jcp/clinical-outcomes-intravenous-ketamine-for-depression-va-health-system/) and multiple ketamine treatments, only 26% of patients were still responding and only 15% were symptom-free and in remission. In chemical terms, ketamine is a chiral molecule, meaning it has two chemical forms that are mirror images of each other: R-Ketamine and S-Ketamine. Racemic ketamine is a mixture of both R-Ketamine and S-Ketamine in equal parts and is the most commonly used form of ketamine in clinical settings. Ketamine is administered to patients intravenously. During this procedure, patients are closely monitored by a healthcare professional because ketamine is a dissociative drug, which means patients can feel disconnected from reality and engage in dangerous and life-threatening behaviors. In addition, patients may also experience severe side effects, including: Dissociation Intoxication Sedation High blood pressure Dizziness Headache Blurred vision Anxiety Nausea and vomiting A typical treatment plan includes four to six sessions over two to three weeks. Some patients need booster sessions, typically once a month or once every three months, depending on the patient. To boost the effects of ketamine, it is recommended to combine it with a form of psychotherapy, such as cognitive behavioral therapy (CBT). The surge in demand for this drug has paved the way for a cottage industry of clinics offering ketamine treatments. Some companies make sweeping claims that they’re able to treat dozens of conditions, including depression, anxiety, chronic pain, PTSD, bipolar disorder, and migraines. Such claims are currently not backed by scientific studies. As the industry is unregulated, the quality of care received at these clinics [can be highly variable.](https://www.statnews.com/2018/09/24/ketamine-clinics-severe-depression-treatment/) Many clinics are not run by doctors of psychiatry and are simply pain management clinics that have added ketamine to their list of treatments or are spas with staff not trained in mental health treatment. In addition, it can be expensive. Typically, treatments cost between \$400 to \$1,000 per session, which can add up to thousands for the full treatment. If you’re considering this option, our advice is to discuss it with your family doctor before committing to any clinic. Esketamine (Brand Name: Spravato) Ketamine shows some promise in treating treatment-resistant depression, but the IV administration is time-consuming. To overcome these issues, researchers developed a new antidepressant using only the S-ketamine fraction, aptly named Esketamine. In 2019, the FDA approved this product as a nasal spray for easy application, sold under the brand name Spravato. Clinical [studies](https://pubmed.ncbi.nlm.nih.gov/31109201/) have shown that S-ketamine has fast antidepressant effects, with some patients reporting a reduction in symptoms [within](https://psychiatryonline.org/doi/10.1176/appi.ajp.2019.19020172?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%20%200pubmed) hours of administration. This is in contrast to traditional antidepressant medications that can take weeks or months to take effect. This makes it particularly beneficial for patients who have not responded to other treatments or are in urgent need of treatment due to severe suicidal tendencies. After an eight-week treatment, [about](https://www.nejm.org/doi/10.1056/NEJMoa2304145) one third of patients had achieved remission and, of these, about one third had not relapsed more than eight months later. Spravato comes with specific guidelines for administration due to potential side effects such as nausea, headaches, dizziness, disorientation, and dissociation immediately after use. It must be administered at certified treatment centers under the supervision of a mental health care professional. Ideally, esketamine should be used in conjunction with a conventional antidepressant medication. The aim is to use esketamine for fast relief from depression symptoms until the other medication takes effect. In most cases, patients receive esketamine twice a week for the first month, and then if patients improve, they continue to receive the drug at a lower frequency for a few weeks or months. Typically, this means treatments start as weekly, then drop to every two weeks, then monthly, etc. Arketamine Researchers have also tested the R-ketamine fraction — called arketamine — to treat major depression and other mental health conditions, but this drug has not received approval from the FDA yet. [Preliminary](https://pubmed.ncbi.nlm.nih.gov/35977629/) results are encouraging, with antidepressant effects faster and longer than ketamine and fewer side effects, especially in terms of dissociation and hallucinations. Clinical trials are currently underway in the US and other locations around the world. In addition to its antidepressant-like effects, arketamine may help treat patients with various neurological disorders, such as Parkinson's disease and multiple sclerosis. Moreover, [arketamine](https://linkinghub.elsevier.com/retrieve/pii/S0028390822002301) has anti-inflammatory, bronchodilating, and neuroprotective effects, which means it could be a new [drug](https://www.nature.com/articles/s41380-021-01121-1) for patients with neurological disorders and inflammatory diseases. Dextromethorphan-bupropion (Brand Name: Auvelity) A new fast-acting medication called Auvelity was just approved by the US Food and Drug Administration to treat patients with major depressive disorder (MDD). Auvelity is a combination of two already existing drugs: dextromethorphan and bupropion. Dextromethorphan is commonly used in cough syrups to provide temporary relief from cough. Recent [research](https://www.tandfonline.com/doi/abs/10.1080/14728214.2021.1898588) showed it can also be used to alleviate depressive symptoms, but it’s metabolized very quickly in the body. Bupropion is an existing antidepressant medication, which also slows down the metabolism of dextromethorphan in the body. Staying in the body longer means the levels of drugs are more stable and can potentially help patients more. A phase three [clinical trial](https://www.psychiatrist.com/jcp/efficacy-safety-of-axs-05-dextromethorphan-bupropion-mdd/) confirmed that Auvelity can improve symptoms of depression and a few patients started experiencing the benefits after just one week. After six weeks, over 50% of the patients responded to the treatment and were feeling better and 40% were in remission which is a slightly higher remission rate than for other types of antidepressant medications. Crucially, this [combination](https://psychiatryonline.org/doi/full/10.1176/appi.ajp.21080800) works significantly better than bupropion alone. After six weeks, only about 40% of patients responded to bupropion in isolation, and less than 20% achieved remission. Auvelity doesn’t have the same safety restrictions as ketamine, making it a much safer alternative. Typically, it has similar [side effects](https://psychiatryonline.org/doi/full/10.1176/appi.ajp.21080800) and warnings compared to existing antidepressant medications, including dizziness, nausea, dry mouth, decreased appetite, and anxiety. There is a risk that Auvelity may increase suicidal thoughts and actions in young adults, adolescents, and children. For this reason, it’s essential to pay close attention to sudden changes in mood, behavior, thoughts, feelings, or suicidal thoughts when taking this drug. Additionally, Auvelity should not be taken by patients with a history of seizures, or eating disorders, or those taking other antidepressants like monoamine oxidase inhibitors, benzodiazepines, barbiturates, or anti-seizure medicines. Additional Considerations Regarding Traditional Antidepressant Medications As described earlier, most antidepressants take weeks or months for patients to begin experiencing the benefits (if they experience benefits at all). However, there is some [evidence](https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2211759/) that a few antidepressants work faster in some patients but there are no reliable ways to determine which patients will respond faster. These include, for example, some selective serotonin reuptake inhibitors (SSRIs), serotonin-norepinephrine reuptake inhibitors (SNRIs), and tricyclic antidepressants (TCAs). SSRIs and SNRIs aim to increase the levels of serotonin and norepinephrine in the brain. They’re often the first option primary care doctors prescribe because they generally cause fewer side effects. Patients may experience better quality of sleep, higher levels of energy, and increased appetite within the first 1-2 weeks after starting treatment. Improvement in these physical symptoms can be an important early signal that the medication is working. In most cases, severe symptoms may still need up to 6-8 weeks to fully improve. Some common examples of these drugs include: **SSRIs** Citalopram (Celesta) Fluoxetine (Prozac) Sertraline (Zoloft) **SNRIs** Venlafaxine (Effexor) Desvenlafaxine (Pristiq) Duloxetine (Cymbalta) Similarly to SNRIs, tricyclic antidepressants also aim to increase the levels of serotonin and norepinephrine, but they tend to cause more side effects. They’re typically only prescribed for patients who have tried other antidepressants without improvement. One example of a fast-acting tricyclic antidepressant is called desipramine, and [more](https://www.nature.com/articles/1300341.pdf) than 50% of patients experience significant improvements during the first week of treatment. However, it is important to note that response times to antidepressant medications vary greatly from patient to patient, and it is crucial to consult with a healthcare professional to determine the most appropriate treatment approach for an individual’s specific needs. Conclusion The treatment landscape for depression is evolving, with new options providing faster relief and potentially fewer side effects compared to traditional antidepressant medications. Traditional medications often involve a lengthy trial period and can come with unpleasant side effects, with only about one-third of patients having reliable reductions in depression symptoms. Among the newer treatments, TMS stands out for its noninvasiveness and rapid effectiveness. Accelerated fMRI theta burst stimulation, in particular, offers a significant advancement by using fMRI and neuronavigation for precise coil placement, leading to high response and remission rates within a single week of treatment. This method, available at our clinic, is among the most effective fast-acting treatments for depression, with the added advantage of not impairing cognitive functions. Other fast-acting treatments like ketamine, esketamine, and dextromethorphan-bupropion provide rapid symptom relief by targeting neurotransmitters such as glutamate. However, these treatments can come with side effects that patients should consider carefully, and the effects of these treatments are often not long-lasting. Ultimately, the combination of fMRI TMS with cognitive behavioral therapy (CBT) offers a promising solution for many patients with treatment-resistant depression. This integrated approach not only provides rapid symptom relief but also promotes sustained improvement in brain function and overall mental health. *If you are interested in receiving accelerated fMRI TMS therapy at Cognitive FX,* [*click here to learn more*](https://www.cognitivefxusa.com/tms-new-patient-paperwork) *and see if you’re a good fit for treatment.* Cited Research [A reanalysis of the STAR\*D study’s patient-level data with fidelity to the original research protocol](https://pmc.ncbi.nlm.nih.gov/articles/PMC10373710/) [Repetitive transcranial magnetic stimulation treatment for depressive disorders](https://journals.lww.com/co-psychiatry/fulltext/2019/09000/repetitive_transcranial_magnetic_stimulation.8.aspx) [Stanford Neuromodulation Therapy (SNT): A Double-Blind Randomized Controlled Trial](https://psychiatryonline.org/doi/10.1176/appi.ajp.2021.20101429?url_ver=Z39.88-2003&rfr_id=ori%3Arid%3Acrossref.org&rfr_dat=cr_pub++0pubmed) [Antidepressant effects of ketamine in depressed patients](https://www.sciencedirect.com/science/article/abs/pii/S0006322399002309?via%3Dihub) [Efficacy and Safety of Flexibly Dosed Esketamine Nasal Spray Combined With a Newly Initiated Oral Antidepressant in Treatment-Resistant Depression: A Randomized Double-Blind Active-Controlled Study](https://psychiatryonline.org/doi/10.1176/appi.ajp.2019.19020172)
***

### About the author
[Dr. Diane Spangler, Ph.D.](https://www.cognitivefxusa.com/blog/author/dr-diane-spangler-phd)
Dr. Spangler is a Clinical Psychologist with over 20 years of experience working in both clinical and academic settings. She earned her doctorate degree in Clinical Psychology at the University of Oregon followed by a Postdoctoral Research Fellowship in the Department of Psychiatry at the Stanford University School of Medicine. Dr. Spangler served as a Professor of Psychology at Brigham Young University for 15 years where she directed training in Cognitive Behavioral Therapy for the Clinical Psychology Doctoral Program, and conducted research on the etiology and treatment of depressive, anxiety, and eating disorders. She also served as a Visiting Professor in the Department of Psychiatry Cognitive Therapy Centre at Oxford University in England. Dr Spangler has authored over 60 publications and has lectured worldwide. She has received numerous awards for her collective work from the National Institute of Mental Health, the American Psychological Association, the International Association for Cognitive Psychotherapy, the Association for Behavioral and Cognitive Therapies, the Beck Institute, and the National Association of Professional Women. |
| Shard | 90 (laksa) |
| Root Hash | 14321596278185583490 |
| Unparsed URL | com,cognitivefxusa!www,/blog/fast-acting-depression-treatment-options s443 |