ℹ️ Skipped - page is already crawled
| Filter | Status | Condition | Details |
|---|---|---|---|
| HTTP status | PASS | download_http_code = 200 | HTTP 200 |
| Age cutoff | PASS | download_stamp > now() - 6 MONTH | 0.7 months ago |
| History drop | PASS | isNull(history_drop_reason) | No drop reason |
| Spam/ban | PASS | fh_dont_index != 1 AND ml_spam_score = 0 | ml_spam_score=0 |
| Canonical | PASS | meta_canonical IS NULL OR = '' OR = src_unparsed | Not set |
| Property | Value |
|---|---|
| URL | https://link.springer.com/article/10.1007/s15010-026-02768-0 |
| Last Crawled | 2026-03-19 01:29:44 (20 days ago) |
| First Indexed | not set |
| HTTP Status Code | 200 |
| Meta Title | Persistence of Post-Acute COVID-19 Sequelae (PASC) symptoms in healthcare workers four years after ancestral SARS-CoV-2 infection: a prospective multicentre cohort | Infection | Springer Nature Link |
| Meta Description | Post-Acute Sequelae of SARS-CoV-2 Infection (PASC), or long COVID (LC), remains a significant burden for public health, with limited long-term data. This s |
| Meta Canonical | null |
| Boilerpipe Text | Abstract
Purpose
Post-Acute Sequelae of SARS-CoV-2 Infection (PASC), or long COVID (LC), remains a significant burden for public health, with limited long-term data. This study aimed to assess the prevalence and evolution of PASC symptoms after ancestral SARS-CoV-2 (aSCV2) infection in a longitudinal healthcare worker (HCW) cohort.
Methods
A multicentre cohort study involving HCWs from 14 institutions was conducted in Switzerland. Infection status was based on self-reported positive swabs, with additional serology used to confirm uninfected controls. Baseline was defined as the first survey conducted in 2022 (median 18.5 months post-infection), with follow-up surveys every 6 months through November 2024. To identify PASC-specific symptoms, 24 chronic symptoms were compared between 456 aSCV2-infected and 571 uninfected participants using chi-square tests at baseline. In aSCV2-infected individuals reporting PASC-specific symptoms, symptom trajectories and subjective LC were analyzed across follow-up surveys. Functional limitations were assessed using the Post-COVID Functional Status (PCFS) scale.
Results
Thirteen of 24 symptoms were more common in aSCV2-infected individuals, with fatigue (22.8%), loss of smell/taste (11.4%), and brain fog (8.3%) being most prevalent. At baseline, 186/456 (40.8%) infected participants reported ≥ 1 PASC-specific symptom. Most symptoms declined in prevalence up to the last survey (median 47.5 months post-infection), although 41/70 (58.6%) remaining participants still reported ≥ 1 PASC symptom. Subjective LC was reported by 70/186 (37.6%) and was associated with higher symptom burden. PCFS scores showed slight impairments in most cases, although moderate-to-severe limitations often persisted.
Conclusions
PASC symptoms persisted up to four years after aSCV2 infection in a substantial proportion of HCWs.
Similar content being viewed by others
Introduction
Although acute SARS-CoV-2 infection has caused significant mortality and morbidity, attention has increasingly shifted to its long-term effects, commonly referred to as Post-Acute Sequelae of SARS-CoV-2 Infection (PASC) or long COVID (LC). PASC is defined as symptoms that persist or newly develop at least three months after acute infection, last for at least two months, and cannot be explained by alternative diagnoses [
1
,
2
]. It includes a wide range of symptoms affecting multiple organ systems, with fatigue, cognitive dysfunction, and respiratory symptoms being most common [
3
,
4
,
5
,
6
,
7
,
8
,
9
]. However, many of these symptoms also occur in non-infected individuals and are not specific for PASC. Additionally, not all individuals reporting PASC symptoms consider themselves to suffer from LC, highlighting the heterogeneity of post-COVID outcomes and the challenges of their assessment. Prevalence estimates of PASC vary across studies, ranging from 3 to 54%, depending on the PASC definition, population, sampling scheme, severity and time since initial infection, vaccination status, as well as the viral variant [
5
,
8
,
10
,
11
,
12
,
13
,
14
,
15
]. Comparative analyses show that the risk of developing PASC is highest after infection with ancestral SARS-CoV-2 (aSCV2) and decreases with subsequent variants [
5
,
8
,
13
].
During the aSCV2-dominant period of the pandemic, health care workers (HCWs) were particularly affected by PASC due to their increased exposure to SARS-CoV-2, with prevalence rates noticeably higher than those observed in the general population [
13
,
14
,
16
,
17
,
18
]. Analysis of PASC trajectories in the general population showed a decline in prevalence, especially during the first year after infection [
15
,
19
,
20
]. Nevertheless, a substantial proportion of individuals (18–47%) continued to experience PASC symptoms two years post-infection [
15
,
20
,
21
]. Thereafter, available data is limited, especially among HCWs, although recent studies indicate a relevant ongoing burden of disease [
11
,
22
,
23
,
24
,
25
].
To guide post-COVID-19 care and occupational health strategies, this study aims to identify PASC-specific symptoms and to investigate the evolution of PASC symptoms in HCWs up to four years after aSCV2 infection. We also compare individuals with and without subjective LC in terms of PASC symptomatology and assess changes in subjective LC and the associated limitations in daily living over time, for a more comprehensive understanding of both the clinical and self-perceived long-term impact of COVID-19.
Methods
Setting and participants
In 2022, a longitudinal multicentre cohort involving HCWs from 14 institutions in northeastern Switzerland was launched. Employees aged ≥ 16 years of any work type, with or without direct patient contact, were eligible for inclusion and all participants provided electronic informed consent. The study protocol was approved by the Ethics Committee of Eastern Switzerland (#2020–00502).
Data collection
Serological testing
Serological testing for anti-spike (anti-S) and anti-nucleocapsid (anti-N) antibodies was performed in May/June 2022 in all participants to identify asymptomatic infections [
26
]. The antibodies were measured using the Roche Elecsys electrochemiluminescence immunoassay (Roche Diagnostics, Rotkreuz, Switzerland).
Baseline survey
At baseline (September 2022), data were collected through an electronic baseline questionnaire including questions on personal health, occupational and non-occupational exposures, SARS-CoV-2 infection and vaccination history.
Follow-up surveys
Follow-up surveys were conducted approximately every 6 months (March to April 2023, October to November 2023, April to May 2024, October to November 2024). In those questionnaires, participants indicated the presence and duration of PASC-compatible symptoms as well as whether they suffer from LC (ongoing, resolved, never experienced). Additionally, SARS-CoV-2 infection and vaccination status were regularly updated.
Definitions
Infection status
Participants were classified as aSCV2-infected if they reported a positive SARS-CoV-2 swab between February 2020 and January 2021 [
27
]. Participants were assigned to the uninfected control group if they reported no previous SARS-CoV-2 infection and had a negative anti-N antibody result in June 2022. Thus, participants with a positive swab after January 2021 or positive anti-N antibody results in June 2022 were excluded, ensuring that only aSCV2-infected and uninfected participants were included, while individuals infected with later viral variants were not considered. Potential reinfections after the initial aSCV2 infection were not considered, as testing for SARS-CoV-2 was no longer recommended by the Swiss Federal Office of Public Health after February 2022, leading to incomplete detection of later infections [
28
]. Validation of self-reported swab results with data from the division of occupational medicine (performed in the largest participating hospital) showed excellent concordance [
29
].
PASC symptoms
The 24 symptoms included in the surveys were selected based on national SARS-CoV-2 testing recommendations during the early phase of the pandemic. The symptoms were: Fatigue, Loss of Smell/Taste, Brain Fog, Joint Pain, Hair Loss, Headache, Chest Pain, Muscle Pain, Shortness of Breath, Dizziness, Cough, Burnout or Exhaustion, Runny Nose, Fever, Sneezing, Sore Throat, Abdominal Pain, Loss of Appetite/Nausea, Chills or Shivering, Red or Itchy Eyes, Erectile Dysfunction, Diarrhea, Menstrual Complaints and Rash. Testing for SARS-CoV-2 in individuals with compatible symptoms, using either rapid antigen tests or polymerase chain reaction, was recommended and later became mandatory for access to public institutions, including hospitals, in Switzerland. Symptoms that were described as chronic (i.e., longer than 7 days) and had emerged after the start of the COVID-19 pandemic were considered as PASC-related. Indications of symptoms that were either acute or chronic with onset before the pandemic were assigned as being non-PASC-compatible.
Subjective LC and functional limitations
Subjective LC was based on participants’ self-assessment; no further diagnostic criteria were applied. Those self-reporting LC were asked to grade their attributed functional limitations using the PCFS, a scale used to assess the needs for rehabilitation or recovery in COVID-19 patients. It differentiates: 0 = no functional limitations, 1 = symptoms without significant impact on daily life, 2 = slight limitations of usual activities, 3 = substantial restrictions with reduced everyday functioning, and 4 = severe limitations with dependence on assistance for activities of daily living [
30
].
Study design
The study design entailed a cross-sectional and a longitudinal analysis. In the cross-sectional analysis, PASC-specific symptoms were identified by comparing aSCV2-infected and uninfected individuals. In the longitudinal analysis, trajectories of symptoms, LC and PCFS were analyzed in aSCV2-infected participants that reported at least one PASC symptom at baseline (Fig.
1
).
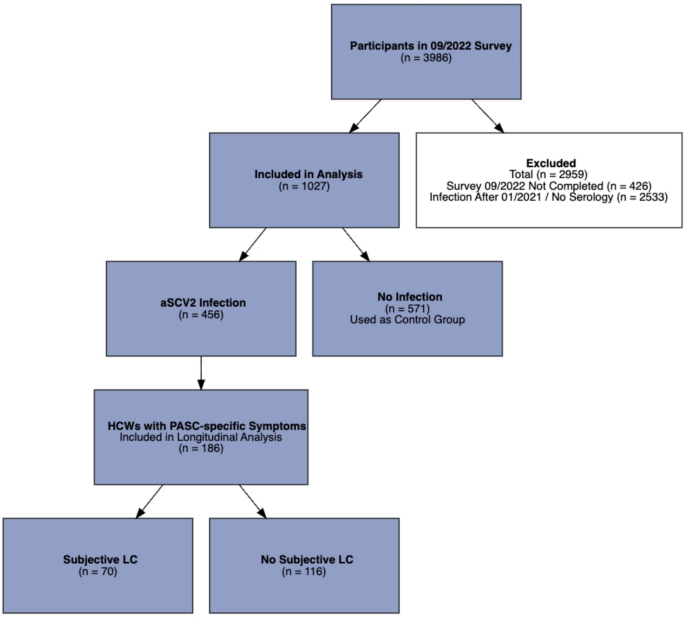
Fig. 1
Study Flow showing the process of enrolment and allocation to the different groups. N = Number of Participants, HCWs = Health Care Workers, LC = long COVID, PASC = Post-Acute COVID-19 Sequelae, aSCV2 = ancestral SARS-CoV-2
Full size image
Statistical analysis
For the cross-sectional analysis, demographic and clinical characteristics between aSCV2-infected participants and the uninfected controls were compared using descriptive statistics. We calculated p-values using the Wilcoxon rank-sum test for continuous variables and the chi-square test or Fisher’s exact test for categorical variables. To distinguish PASC-specific symptoms from non-specific symptoms, the chi-square test was used; symptoms being significantly more common in the aSCV2 group were considered PASC-specific. Furthermore, baseline characteristics, symptom counts, and symptom prevalence were compared between participants with and without subjective LC using the same methods as described for aSCV2- and uninfected participants.
For the longitudinal analysis, we calculated the prevalence (for binary outcomes) and the median (for continuous outcomes) at every time point. Alluvial plots were used, where appropriate, to visualize how individuals move across categories over time. The independent effect of time on the number of symptoms and on the prevalence of the three most common symptoms (fatigue, brain fog and loss of smell/taste) was assessed using negative binomial (for symptom count) and logistic regression analysis (for symptoms). Time points were included as categorical and not as a continuous variable, as the effect of time was assumed to be non-linear. To account for repeated measurements, mixed-effects models with a random intercept for each individual were used. Adjusted incidence rate ratios (aIRR) from the negative binomial regression and adjusted odds ratios (aOR) from the logistic regression for the different time points, along with corresponding 95% confidence intervals (CI) were calculated. The models were adjusted for a priori defined covariates, namely age, sex, and Body-Mass-Index (BMI). To account for attrition bias, sensitivity analyses were performed: one restricted to participants with complete data across all surveys and another by adding the number of observed time points per participant to the negative binomial regression model. Spearman’s rank correlation was used to assess the association between baseline and last follow-up values of PCFS and total symptom count.
Statistical significance was set at a p-value of < 0.05. All statistical analyses and figures were created using R version 4.4.2 (2024–10-31); descriptive statistics were performed using “gtsummary”, for regression analyses the package “lme4” was used and correlation analyses were carried out using Base R.
Results
Study population
Of 3,986 HCWs who completed the survey in September 2022, 1,027 (25.8%) were included in the baseline analysis (median age: 44 years; 80.6% women), of whom 456 (44.4%) were aSCV2-infected and 571 (55.6%) were uninfected controls. A total of 2,959 participants were excluded due to infections during later pandemic phases or incomplete baseline surveys (Fig.
1
; Supplementary Material Table S1).
Compared to controls, aSCV2-infected participants were younger (median age 41 vs. 47 years, p < 0.001), more frequently employed as nurses (59.4% vs. 37.5%, p < 0.001) and had children under age 6 at home (13.6% vs. 9.3%, p = 0.029), while a smaller proportion were smokers (13.6% vs. 21.4%, p = 0.001) (Table
1
). The median time from the first positive SARS-CoV-2 test to the baseline survey was 18.5 months and 47.5 months to the last survey (Supplementary Material Table S2).
Table 1 Characteristics of the aSCV2-Infected Group Compared with the Non-Infected Control Group at Baseline (09/2022)
Full size table
Identification of PASC-specific symptoms and subjective LC
Among 24 potential PASC symptoms, 13 symptoms were significantly more common in the aSCV2 group, with fatigue (22.8% in aSCV2-infected and 7.4% in controls), loss of smell/taste (11.4% and 0.4%), and brain fog (8.3% and 1.8%) being the most frequent (Fig.
2
; Supplementary Material Table S3).
Fig. 2
Absolute difference in symptom prevalence (%) between the ancestral SARS CoV-2 (aSCV2) infected group and the non-infected control group at baseline (09/2022) represented as dots, with 95% confidence intervals. Orange = PASC-specific symptoms; blue = non-specific symptoms
Full size image
Among HCWs with PASC-specific symptoms at baseline (n = 186/1027, 18.1%), 38% (n = 70) self-reported having LC, while 62% (n = 116) did not (anymore). Participants with subjective LC at baseline had a higher median number of symptoms compared to those without subjective LC (4 vs 1) (Table S4).
Trajectory of symptoms
Out of 456 aSCV2-infected participants, 40.8% (n = 186) reported at least one PASC-specific symptom and were included in the longitudinal analysis. Participants completed a median of 3 surveys (range 1–5). Overall, 72.0% (n = 134) did not have complete data or were lost to follow-up during the course of the study. Compared to those with complete data, these participants were younger (median age 39 vs. 47.5 years), more often male (14.9% vs. 23.1%), more commonly smokers (11.9% vs. 5.8%) and more frequently working full-time (45.5% vs. 34.6%). Additionally, they were less likely to report comorbidities other than pollen allergy (33.3% vs. 58.6%) (Supplementary Material Table S5).
The median number of symptoms declined from 2 at baseline to 0 symptoms in the last survey, and from 2 to 1 in participants with complete data (n = 52); the decline was most pronounced from the baseline to the first follow-up survey and remained mostly stable thereafter (Fig.
3
; Supplementary Material Table S6). In the last survey (median 47.5 months after infection), 58.6% of all participants (59.6% of participants with complete data) still reported ≥ 1 PASC symptom, with fatigue being the most persistent symptom (35.7%) (Supplementary Material Table S7/ Table S8). For those with complete data, participants with an initially high number of symptoms tended to also have higher symptom scores in the last survey (Spearman’s ρ = 0.338, p = 0.014) (Fig.
3
; Supplementary Material Figure S1).
Fig. 3
A
displays the count of symptoms for each time point, grouped as described in the legend, for all participants including participants that dropped out (n=186). The dashed black line and error bars represent the adjusted incidence rate ratio (aIRR) and 95% confidence intervals for symptom count, referenced to baseline (09/2022).
B
shows longitudinal trajectories of symptom groups among participants with complete data at every time point (n=52), with the black solid line indicating the median number of symptoms at each time point
Full size image
Assessment of symptom trajectories using the negative binomial mixed-effects model showed a significant decline in the number of symptoms per participant at the last survey compared to baseline (aIRR 0.71, 95% CI 0.58–0.87, p = 0.001). Results were similar with complete case analysis (aIRR = 0.72, 95% CI 0.56–0.93, p = 0.013) (Supplementary Material Table S9).
For the three most prevalent symptoms, fatigue decreased from 55.9% (104/186) to 35.7% (25/70) (aOR 0.23, 95% CI 0.10–0.52, p < 0.001), loss of smell/taste from 28.0% (52/186) to 18.6% (13/70) (aOR 0.03, 95% CI 0.00–0.21, p < 0.001) and brain fog changed from 20.4% (38/186) to 14.3% (10/70) without being significant (aOR 0.96, 95% CI 0.27–3.37, p = 0.95) (Fig.
4
). Figures were similar in the subset of participants with complete data (Supplementary Material Figure S2; Table S10).
Fig. 4
Bar graphs showing the prevalence of the three most prevalent PASC-specific symptoms (Fatigue, Brain Fog, Loss of Smell/ Taste) in participants with available data at each follow-up time point. The black line shows the adjusted Odds Ratio (aOR) with 95% confidence intervals for symptom presence at each time point (relative to baseline), shown as error bars. Sample size: 09/2022: n=186, 03/2023: n=124, 10/2023: n=105, 04/2024: n=83, 10/2024: n=70
Full size image
Trajectory of subjective LC and functional status
77 of the 456 aSCV2-infected participants reported LC at baseline. To ensure consistency with the longitudinal symptom trajectory analyses, only participants reporting ≥ 1 PASC-specific chronic symptom were included. In this subgroup, 70 of 186 individuals reported subjective LC, of whom 12.9% (9/70) reported resolution of symptoms at the first follow-up. Thereafter, there were no new reports of resolved symptoms. At the final follow-up, only 18 of the initial 70 participants remained, with 14 indicating ongoing subjective LC (Supplementary Material Figure S3; Table S11).
When analyzing the PCFS score at baseline, 71.4% (n = 50) of participants with subjective LC had no or minor (PCFS 0 or 1) limitations in their daily life. This figure remained stable over time as did the median PCFS. Participants with moderate or severe limitations (PCFS score ≥ 2) at baseline tended to still report limitations at the final follow-up (Spearman’s ρ = 0.40, p = 0.10). However, data availability declined over follow-up due to decreasing subjective LC reports and participant attrition (Supplementary Material Figures S4, S5; Table S12).
Discussion
In a prospective multicentre cohort of HCWs, we demonstrate a non-linear decline in PASC-specific symptoms over time, with up to 60% of individuals still reporting symptoms after a median of almost 4 years after aSCV2 infection. Fatigue, brain fog, and loss of smell or taste are the most prevalent symptoms. For those with subjective LC, the limitations in daily life are mostly mild, but often persist over time.
The prevalence of PASC symptoms at baseline was 40.8% (median 18.5 months post-infection), which is higher than reported in prior studies [
15
,
31
,
32
]. A recent meta-analysis including only studies with more than 3 years of follow-up, showed a pooled prevalence of 20% at 3 years, again lower than our findings (67% at 3 years). However, the individual studies contributing to this analysis showed a wide range of prevalence estimates (6–54%) [
22
]. One factor for this difference could be the high exposure of our cohort during the aSCV2 period compared to non-HCWs, as this viral variant was shown to have the highest PASC incidence one year post-infection, with declining rates observed for later variants [
8
]. Consistent with previous reports of neurological symptoms persisting, brain fog showed no significant decline, suggesting ongoing cognitive impairment in PASC affected patients [
15
,
33
].
In our cohort, self-reported LC was associated with a higher number of symptoms and specific symptoms, most notably fatigue (80% vs. 41% without LC), which is in line with previous findings [
34
,
35
,
36
]. Gottlieb et al. had a similar design with self-reported LC through continuous surveys. In a cross-sectional analysis up to 40 months post-infection, only 2% reported resolved LC and only 26% of participants with current LC reported improved symptoms [
24
]. This persistence of LC is consistent with our analysis of subjective LC prevalence, where no participants reported resolved symptoms after the first follow-up and the trend in functional limitations (PCFS), where only a small subset reported complete resolution of limitations.
Our findings indicate that full recovery from PASC remains uncertain for many patients and functional limitations persist. PASC should be recognized as a chronic condition requiring long-term clinical and social support, and further research has to be supported to clarify the pathophysiology and to identify diagnostic markers and effective treatment. As our cohort consists of HCWs, these findings underline the need for occupational health strategies, including structured return-to-work programs and flexible workload adjustments, to support sustainable reintegration and minimize the loss of essential workforce.
Limitations
This study has several limitations. First, prior infection status was partially based on anti-N antibody negativity. We acknowledge that some previously infected individuals may have been misclassified due to absent seroconversion or declining antibody levels over time, which may have led to misclassification in the cross-sectional analysis and to over- or underestimation of symptom prevalence across time points [
37
]. To minimize this risk, we not only required anti-N negativity for classification into the uninfected control group, but also the absence of a documented positive SARS-CoV-2 test. Given the extensive and partly mandatory testing policies for HCWs until February 2022, we consider the likelihood of undetected infections in our cohort to be low.
Second, information bias due to self-reported data may have caused misclassification and over- or underestimation of prevalence rates.
Third, substantial loss to follow-up limited the size of the dataset and potentially introduced attrition bias, causing an underestimation of PASC-prevalence if affected participants were less likely to remain in the study. However, sensitivity analyses focusing on participants with complete data and a model adjusted for the number of answered surveys mostly confirmed our results. Although regression models were adjusted for age, sex, and BMI, residual confounding by unmeasured factors, such as pre-existing comorbidities, mental health status, or occupational stress is possible. These factors may have influenced both the likelihood of infection and the reporting of persistent symptoms, potentially leading to over- or underestimation of the observed outcomes. In addition, effect modification by baseline health status or pre-existing comorbidities cannot be ruled out.
Fourth, survivor bias cannot be excluded. Only individuals who survived aSCV2 infection and remained in the workforce until 2022 were eligible for inclusion. Individuals who experienced severe outcomes, left the workforce due to functional impairment, or died were not captured, which may have led to an underestimation of the true long-term burden of PASC.
Fifth, reinfections were not assessed, as mandatory SARS-CoV-2 testing in Switzerland was discontinued in February 2022; undetected reinfections may therefore have biased symptom trajectories [
28
].
Finally, the transferability of our findings to the general population is limited, as HCWs may differ in exposure risk and health-seeking behavior.
Strengths of this study include clearly defined infection groups through serology and timing, and a unique follow-up period providing data up to four years post-infection. Furthermore, PCFS scoring allowed assessment of functional limitations over time.
This study provides four-year follow-up data on PASC in a predominantly young and healthy cohort. Despite a general decline in symptom prevalence, key symptoms such as fatigue, brain fog, and loss of smell or taste persisted in a substantial subset up to four years post-aSCV2 infection. Long-term follow-up and tailored care strategies appear essential for managing persistent PASC symptoms.
Data availability
All data generated or analysed during this study are included in this published article and its Supplementary Material.
References
Post COVID-19 condition (Long COVID) [Internet].
https://www.who.int/europe/news-room/fact-sheets/item/post-covid-19-condition
. Accessed 15 Jan 2025.
Parums DV. Long COVID or Post-Acute Sequelae of SARS-CoV-2 Infection (PASC) and the urgent need to identify diagnostic biomarkers and risk factors. Med Sci Monit. 2024.
https://doi.org/10.12659/MSM.946512
.
Article
PubMed
PubMed Central
Google Scholar
Davis HE, McCorkell L, Vogel JM, Topol EJ. Long COVID: major findings, mechanisms and recommendations. Nat Rev Microbiol. 2023;21:133–46.
https://doi.org/10.1038/s41579-022-00846-2
.
Article
CAS
PubMed
PubMed Central
Google Scholar
Reese JT, Blau H, Casiraghi E, Bergquist T, Loomba JJ, Callahan TJ, et al. Generalisable long COVID subtypes: findings from the NIH N3C and RECOVER programmes. EBioMedicine. 2023;87:104413.
https://doi.org/10.1016/j.ebiom.2022.104413
.
Article
PubMed
Google Scholar
Thaweethai T, Jolley SE, Karlson EW, Levitan EB, Levy B, McComsey GA, et al. Development of a definition of postacute sequelae of SARS-CoV-2 infection. JAMA. 2023;329:1934.
https://doi.org/10.1001/jama.2023.8823
.
Article
CAS
PubMed
PubMed Central
Google Scholar
Griffin DO. Postacute sequelae of COVID (PASC or Long COVID): an evidenced-based approach. Open Forum Infect Dis. 2024;11:ofae462.
https://doi.org/10.1093/ofid/ofae462
.
Article
PubMed
PubMed Central
Google Scholar
Hastie CE, Lowe DJ, McAuley A, Mills NL, Winter AJ, Black C, et al. True prevalence of long-COVID in a nationwide, population cohort study. Nat Commun. 2023;14:7892.
https://doi.org/10.1038/s41467-023-43661-w
.
Article
CAS
PubMed
PubMed Central
Google Scholar
Xie Y, Choi T, Al-Aly Z. Postacute sequelae of SARS-CoV-2 infection in the Pre-Delta, Delta, and Omicron eras. N Engl J Med. 2024;391:515–25.
https://doi.org/10.1056/NEJMoa2403211
.
Article
CAS
PubMed
PubMed Central
Google Scholar
Sherif ZA, Gomez CR, Connors TJ, Henrich TJ, Reeves WB, RECOVER Mechanistic Pathway Task Force. Pathogenic mechanisms of post-acute sequelae of SARS-CoV-2 infection (PASC). Elife. 2023;12:e86002.
https://doi.org/10.7554/eLife.86002
.
Article
CAS
PubMed
PubMed Central
Google Scholar
Mandel H, Yoo YJ, Allen AJ, Abedian S, Verzani Z, Karlson EW, et al. Long COVID incidence proportion in adults and children between 2020 and 2024: an EHR-based study from the RECOVER initiative. Clin Infect Dis. 2025.
https://doi.org/10.1093/cid/ciaf046
.
Article
PubMed
PubMed Central
Google Scholar
Cai M, Xie Y, Topol EJ, Al-Aly Z. Three-year outcomes of post-acute sequelae of COVID-19. Nat Med. 2024;30:1564–73.
https://doi.org/10.1038/s41591-024-02987-8
.
Article
CAS
PubMed
PubMed Central
Google Scholar
Groff D, Sun A, Ssentongo AE, Ba DM, Parsons N, Poudel GR, et al. Short-term and long-term rates of postacute sequelae of SARS-CoV-2 infection: a systematic review. JAMA Netw Open. 2021;4:e2128568.
https://doi.org/10.1001/jamanetworkopen.2021.28568
.
Article
PubMed
PubMed Central
Google Scholar
Kahlert CR, Strahm C, Güsewell S, Cusini A, Brucher A, Goppel S, et al. Post-acute sequelae after Severe Acute Respiratory Syndrome Coronavirus 2 infection by viral variant and vaccination status: a multicenter cross-sectional study. Clin Infect Dis. 2023;77:194–202.
https://doi.org/10.1093/cid/ciad143
.
Article
PubMed
PubMed Central
Google Scholar
Dörr T, Strahm C, Güsewell S, Ballouz T, Kocan E, Cusini A, et al. Burden of post–acute COVID-19 sequelae in healthcare workers and its course over a 30-month period–results from a prospective multicentre cohort. Infection. 2024.
https://doi.org/10.1007/s15010-024-02418-3
.
Article
PubMed
PubMed Central
Google Scholar
Ballouz T, Menges D, Anagnostopoulos A, Domenghino A, Aschmann HE, Frei A, et al. Recovery and symptom trajectories up to two years after SARS-CoV-2 infection: population based, longitudinal cohort study. BMJ. 2023;381:e074425.
https://doi.org/10.1136/bmj-2022-074425
. (
British Medical Journal Publishing Group;
).
Article
CAS
PubMed
PubMed Central
Google Scholar
Foulkes S, Evans J, Neill C, Bishop J, Khawam J, Islam J, et al. Prevalence and impact of persistent symptoms following SARS-CoV-2 infection among healthcare workers: a cross-sectional survey in the SIREN cohort. J Infect. 2024;89:106259.
https://doi.org/10.1016/j.jinf.2024.106259
.
Article
PubMed
Google Scholar
Lim SH, Lim YC, Zaki RA, Johari BM, Chang CY, Omar SFS, et al. Prevalence and predictors of post-acute COVID syndrome among infected healthcare workers at University Malaya Medical Centre. PLoS ONE. 2024;19:e0298376.
https://doi.org/10.1371/journal.pone.0298376
.
Article
CAS
PubMed
PubMed Central
Google Scholar
Dempsey B, Blake HA, Madan I, Stevelink SAM, Greenberg N, Raine R, et al. Post COVID-19 syndrome among 5248 healthcare workers in England: longitudinal findings from NHS CHECK. Occup Environ Med. 2024;81:471–9.
https://doi.org/10.1136/oemed-2024-109621
.
Article
PubMed
PubMed Central
Google Scholar
Bowe B, Xie Y, Al-Aly Z. Postacute sequelae of COVID-19 at 2 years. Nat Med. 2023;29:2347–57.
https://doi.org/10.1038/s41591-023-02521-2
.
Article
CAS
PubMed
PubMed Central
Google Scholar
Hurme A, Viinanen A, Teräsjärvi J, Jalkanen P, Feuth T, Löyttyniemi E, et al. Post-COVID-19 condition in prospective inpatient and outpatient cohorts. Sci Rep. 2025;15:6925.
https://doi.org/10.1038/s41598-025-90819-1
.
Article
CAS
PubMed
PubMed Central
Google Scholar
Pfrommer LR, Diexer S, Klee B, Massag J, Gottschick C, Purschke O, et al. Post-COVID recovery is faster after an infection with the SARS-CoV-2 Omicron variant: a population-based cohort study. Infection. 2025;53:657–65.
https://doi.org/10.1007/s15010-024-02438-z
.
Article
CAS
PubMed
Google Scholar
Rahmati M, Udeh R, Kang J, Dolja‐Gore X, McEvoy M, Kazemi A, et al. Long‐term sequelae of COVID‐19: a systematic review and meta‐analysis of symptoms 3 years post‐SARS‐CoV‐2 infection. J Med Virol. 2025;97:e70429.
https://doi.org/10.1002/jmv.70429
.
Article
CAS
PubMed
PubMed Central
Google Scholar
Vallée G, Xi D, Avramovic G, O’Kelly B, Lambert JS. Evaluating the longitudinal physical and psychological health effects of persistent long Covid 3.5 years after infection. PLoS ONE. 2025;20:e0326790.
https://doi.org/10.1371/journal.pone.0326790
.
Article
CAS
PubMed
PubMed Central
Google Scholar
Gottlieb M, Yu H, Chen J, Spatz ES, Gentile NL, Geyer RE, et al. Differences in Long COVID severity by duration of illness, symptom evolution, and vaccination: a longitudinal cohort study from the INSPIRE group. Lancet Reg Health Am. 2025;44:101026.
https://doi.org/10.1016/j.lana.2025.101026
.
Article
PubMed
PubMed Central
Google Scholar
Ballouz T, Kerksieck P, Haile SR, Dressel H, Hämmig O, Bauer GF, et al. Work ability trajectories and sick leave in individuals with post COVID-19 condition: 3-year follow-up of a population-based cohort. Lancet Reg Health Eur. 2026;61:101536.
https://doi.org/10.1016/j.lanepe.2025.101536
.
Article
PubMed
Google Scholar
Kahlert CR, Persi R, Güsewell S, Egger T, Leal-Neto OB, Sumer J, et al. Non-occupational and occupational factors associated with specific SARS-CoV-2 antibodies among hospital workers – a multicentre cross-sectional study. Clin Microbiol Infect. 2021;27:1336–44.
https://doi.org/10.1016/j.cmi.2021.05.014
.
Article
CAS
PubMed
PubMed Central
Google Scholar
Federal Office of Public Health. Virus variants overview. [Internet]. [cited 2025 Apr 21].
https://www.covid19.admin.ch/en/epidemiologic/virus-variants
. Accessed 21 Apr 2025.
Coronavirus: Key Decisions of the Federal Council [Internet]. [cited 2025 May 2].
https://www.uvek.admin.ch/uvek/de/home/uvek/coronavirus/wichtige-entscheide.html
. Accessed 2 May 2025.
Kohler P, Güsewell S, Seneghini M, Egger T, Leal O, Brucher A, et al. Impact of baseline SARS-CoV-2 antibody status on syndromic surveillance and the risk of subsequent COVID-19—a prospective multicenter cohort study. BMC Med. 2021;19:270.
https://doi.org/10.1186/s12916-021-02144-9
.
Article
CAS
PubMed
PubMed Central
Google Scholar
Klok FA, Boon GJAM, Barco S, Endres M, Geelhoed JJM, Knauss S, et al. The Post-COVID-19 Functional Status scale: a tool to measure functional status over time after COVID-19. Eur Respir J. 2020;56:2001494.
https://doi.org/10.1183/13993003.01494-2020
.
Article
CAS
PubMed
PubMed Central
Google Scholar
Fernandez-de-las-Peñas C, Notarte KI, Macasaet R, Velasco JV, Catahay JA, Ver AT, et al. Persistence of post-COVID symptoms in the general population two years after SARS-CoV-2 infection: a systematic review and meta-analysis. J Infect. 2024;88:77–88.
https://doi.org/10.1016/j.jinf.2023.12.004
.
Article
PubMed
Google Scholar
Kim Y, Bae S, Chang H-H, Kim S-W. Long COVID prevalence and impact on quality of life 2 years after acute COVID-19. Sci Rep. 2023;13:11207.
https://doi.org/10.1038/s41598-023-36995-4
.
Article
CAS
PubMed
PubMed Central
Google Scholar
Nguyen NN, Tissot-Dupont H, Brouqui P, Gautret P. Post-COVID syndrome in symptomatic COVID-19 patients: a retrospective cohort study. BMC Infect Dis. 2025;25:1099.
https://doi.org/10.1186/s12879-025-11360-0
.
Article
PubMed
PubMed Central
Google Scholar
Danesh V, Arroliga AC, Bourgeois JA, Boehm LM, McNeal MJ, Widmer AJ, et al. Symptom clusters seen in adult COVID-19 recovery clinic care seekers. J Gen Intern Med. 2023;38:442–9.
https://doi.org/10.1007/s11606-022-07908-4
.
Article
PubMed
Google Scholar
Huiberts AJ, De Bruijn S, Andeweg SP, Hoeve CE, Schipper M, De Melker HE, et al. Prospective cohort study of fatigue before and after SARS-CoV-2 infection in the Netherlands. Nat Commun. 2025;16:1923.
https://doi.org/10.1038/s41467-025-56994-5
.
Article
CAS
PubMed
PubMed Central
Google Scholar
Strahm C, Seneghini M, Güsewell S, Egger T, Leal-Neto O, Brucher A, et al. Symptoms compatible with long coronavirus disease (COVID) in healthcare workers with and without severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection—results of a prospective multicenter cohort. Clin Infect Dis. 2022;75:e1011–9.
https://doi.org/10.1093/cid/ciac054
.
Article
PubMed
PubMed Central
Google Scholar
Nakagama Y, Komase Y, Kaku N, Nitahara Y, Tshibangu-Kabamba E, Tominaga T, et al. Detecting waning serological response with commercial immunoassays: 18-month longitudinal follow-up of anti-SARS-CoV-2 Nucleocapsid antibodies. Microbiol Spectr. 2022;10:e00986-22.
https://doi.org/10.1128/spectrum.00986-22
.
Article
CAS
PubMed
PubMed Central
Google Scholar
Download references
Acknowledgements
The SURPRISE+ Study Group: Alexia Cusini, Cantonal Hospital Graubuenden, Chur, Switzerland; Tamara Dörr, HOCH, Cantonal Hospital St.Gallen, Division of Infectious Diseases, Infection Prevention and Travel Medicine, St.Gallen, Switzerland; Stephan Goppel, Psychiatry Services of the Canton of St Gallen, St Gallen, Switzerland; Fabian Grässli, HOCH, Cantonal Hospital St.Gallen, Division of Infectious Diseases, Infection Prevention and Travel Medicine, St.Gallen, Switzerland, Christian R. Kahlert; HOCH, Cantonal Hospital St.Gallen, Division of Infectious Diseases, Infection Prevention and Travel Medicine, St.Gallen, Switzerland and Department of InfectiousDiseases and Hospital Epidemiology, Children’s Hospital of EasternSwitzerland,St. Gallen, Switzerland; Joelle Keller, Hirslanden Clinic Zurich, Zurich, Switzerland; Simone Kessler, HOCH, Cantonal Hospital St.Gallen, Division of Infectious Diseases, Infection Prevention and Travel Medicine, St.Gallen, Switzerland; Philipp Kohler, HOCH, Cantonal Hospital St.Gallen, Division of Infectious Diseases, Infection Prevention and Travel Medicine, St.Gallen, Switzerland and Epidemiology, Biostatistics and Prevention Institute (EBPI), University of Zurich, Zurich, Switzerland; Stefan P. Kuster, HOCH, Cantonal Hospital St.Gallen, Division of Infectious Diseases, Infection Prevention and Travel Medicine, St.Gallen, Switzerland; J. Carsten Möller, Center for Neurological Rehabilitation Zihlschlacht, Zihlschlacht, Switzerland; Maja F. Müller, Hirslanden Clinic Zurich, Zurich, Switzerland; Philip Rieder, Hirslanden Clinic Zurich, Zurich, Switzerland; Lorenz Risch, Labormedizinisches Zentrum Dr Risch Ostschweiz AG, Buchs, Switzerland, Private Universität im Fürstentum Liechtenstein, Triesen, Liechtenstein and Center of Laboratory Medicine, Institute of Clinical Chemistry, University of Bern, Inselspital, Bern, Switzerland; Markus Rütti, HOCH, Hospital Wil, Division of Internal Medicine, St. Gallen, Switzerland; Matthias Schlegel, HOCH, Cantonal Hospital St.Gallen, Division of Infectious Diseases, Infection Prevention and Travel Medicine, St.Gallen, Switzerland; Reto Stocker, Hirslanden Clinic Zurich, Zurich, Switzerland and Foundation Quality of Life, Zurich, Switzerland; Matthias von Kietzell, Hirslanden Clinic Stephanshorn, St. Gallen, Switzerland; Danielle Vuichard-Gysin, Thurgau Hospital Group, Division of Infectious Diseases and Hospital Epidemiology, Muensterlingen and Frauenfeld, Switzerland; Department of Research and Development, Swiss National Centre for Infection Prevention (Swissnoso), Bern, Switzerland; Geriatric Clinic St. Gallen, St. Gallen, Switzerland.
Funding
This work was supported by the Swiss National Sciences Foundation SNSF (grant number 31CA30_196544; grant number PZ00P3_179919 to PK).
Author information
Author notes
Tamara Dörr and Philipp Kohler equal contribution as last authors.
Authors and Affiliations
Division of Infectious Diseases, Infection Prevention and Travel Medicine, HOCH, Cantonal Hospital St.Gallen, Rorschacher Strasse 95, 9007, St. Gallen, Switzerland
Christian R. Kahlert, Stefan P. Kuster, Matthias Schlegel, Carol Strahm, Tamara Dörr & Philipp Kohler
Epidemiology, Biostatistics and Prevention Institute (EBPI), University of Zurich, Hirschengraben 84, 8001, Zurich, Switzerland
Philipp Saurer, Tala Ballouz, Sarah R. Haile, Milo A. Puhan & Philipp Kohler
Cantonal Hospital Graubuenden, Chur, Switzerland
Alexia Cusini
Hirslanden Clinic Stephanshorn, St. Gallen, Switzerland
Matthias von Kietzell
Division of Internal Medicine, HOCH, Hospital Wil, St. Gallen, Switzerland
Markus Rütti
Hirslanden Clinic Zurich, Zurich, Switzerland
Reto Stocker
Division of Infectious Diseases and Hospital Epidemiology, Thurgau Hospital Group, Muensterlingen, Frauenfeld, Switzerland
Danielle Vuichard-Gysin
Department of Research and Development, Swiss National Centre for Infection Prevention (Swissnoso), Bern, Switzerland
Danielle Vuichard-Gysin
Department of Infectious Diseases and Hospital Epidemiology, Children’s Hospital of Eastern Switzerland, St. Gallen, Switzerland
Christian R. Kahlert
Labormedizinisches Zentrum Dr Risch Ostschweiz AG, Buchs, Switzerland
Lorenz Risch
Private Universität im Fürstentum Liechtenstein, Triesen, Liechtenstein
Lorenz Risch
Center of Laboratory Medicine, Institute of Clinical Chemistry, University of Bern, Inselspital, Bern, Switzerland
Lorenz Risch
Foundation Quality of Life, Zurich, Switzerland
Reto Stocker
Authors
Philipp Saurer
Tala Ballouz
Alexia Cusini
Sarah R. Haile
Christian R. Kahlert
Matthias von Kietzell
Stefan P. Kuster
Markus Rütti
Matthias Schlegel
Carol Strahm
Reto Stocker
Danielle Vuichard-Gysin
Lorenz Risch
Milo A. Puhan
Tamara Dörr
Philipp Kohler
Consortia
on behalf of
the SURPRISE+ cohort
Alexia Cusini
, Tamara Dörr
, Stephan Goppel
, Fabian Grässli
, Christian R. Kahlert
, Joelle Keller
, Simone Kessler
, Philipp Kohler
, Stefan P. Kuster
, J. Carsten Möller
, Maja F. Müller
, Philip Rieder
, Lorenz Risch
, Markus Rütti
, Matthias Schlegel
, Reto Stocker
, Matthias von Kietzell
& Danielle Vuichard-Gysin
Contributions
All authors contributed to the study conception and design. Data collection was performed by the SURPRISE + Study Group. Data analyses were performed by P.S. The first draft of the manuscript was written by P.S. and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript. T.D. and P.K. contributed equally as last authors.
Corresponding authors
Correspondence to
Philipp Saurer
or
Philipp Kohler
.
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Ethical approval
The study protocol was approved by the Ethics Committee of Eastern Switzerland (#2020–00502).
Consent to participate
All participants provided electronic informed consent.
Rights and permissions
Open Access
This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit
http://creativecommons.org/licenses/by-nc-nd/4.0/
.
Reprints and permissions
About this article
Cite this article
Saurer, P., Ballouz, T., Cusini, A.
et al.
Persistence of Post-Acute COVID-19 Sequelae (PASC) symptoms in healthcare workers four years after ancestral SARS-CoV-2 infection: a prospective multicentre cohort.
Infection
(2026). https://doi.org/10.1007/s15010-026-02768-0
Download citation
Received
:
22 December 2025
Accepted
:
10 March 2026
Published
:
17 March 2026
Version of record
:
17 March 2026
DOI
:
https://doi.org/10.1007/s15010-026-02768-0
Keywords |
| Markdown | [Skip to main content](https://link.springer.com/article/10.1007/s15010-026-02768-0#main)
[](https://link.springer.com/)
[Account](https://link.springer.com/article/10.1007/s15010-026-02768-0)
[Menu](https://link.springer.com/article/10.1007/s15010-026-02768-0#eds-c-header-nav)
[Find a journal](https://link.springer.com/journals/) [Publish with us](https://www.springernature.com/gp/authors) [Track your research](https://link.springernature.com/home/)
[Search](https://link.springer.com/article/10.1007/s15010-026-02768-0#eds-c-header-popup-search)
[Saved research](https://link.springer.com/saved-research)
[Cart](https://order.springer.com/public/cart)
1. [Home](https://link.springer.com/)
2. [Infection](https://link.springer.com/journal/15010)
3. Article
# Persistence of Post-Acute COVID-19 Sequelae (PASC) symptoms in healthcare workers four years after ancestral SARS-CoV-2 infection: a prospective multicentre cohort
- Research
- [Open access](https://www.springernature.com/gp/open-science/about/the-fundamentals-of-open-access-and-open-research)
- Published:
17 March 2026
- (2026)
- [Cite this article](https://link.springer.com/article/10.1007/s15010-026-02768-0#citeas)
You have full access to this [open access](https://www.springernature.com/gp/open-science/about/the-fundamentals-of-open-access-and-open-research) article
[Download PDF](https://link.springer.com/content/pdf/10.1007/s15010-026-02768-0.pdf)
[Save article](https://link.springer.com/article/10.1007/s15010-026-02768-0/save-research?_csrf=2yDLRFUlZM56sL3HmFpNl6DHsnjGZn2n)
[View saved research](https://link.springer.com/saved-research)
[ Infection](https://link.springer.com/journal/15010)
[Aims and scope](https://link.springer.com/journal/15010/aims-and-scope)
[Submit manuscript](https://submission.nature.com/new-submission/15010/3)
Persistence of Post-Acute COVID-19 Sequelae (PASC) symptoms in healthcare workers four years after ancestral SARS-CoV-2 infection: a prospective multicentre cohort
[Download PDF](https://link.springer.com/content/pdf/10.1007/s15010-026-02768-0.pdf)
- [Philipp Saurer](https://link.springer.com/article/10.1007/s15010-026-02768-0#auth-Philipp-Saurer-Aff2)
[ORCID: orcid.org/0009-0005-7056-4412](https://orcid.org/0009-0005-7056-4412)[2](https://link.springer.com/article/10.1007/s15010-026-02768-0#Aff2),
- [Tala Ballouz](https://link.springer.com/article/10.1007/s15010-026-02768-0#auth-Tala-Ballouz-Aff2)[2](https://link.springer.com/article/10.1007/s15010-026-02768-0#Aff2),
- [Alexia Cusini](https://link.springer.com/article/10.1007/s15010-026-02768-0#auth-Alexia-Cusini-Aff3)[3](https://link.springer.com/article/10.1007/s15010-026-02768-0#Aff3),
- [Sarah R. Haile](https://link.springer.com/article/10.1007/s15010-026-02768-0#auth-Sarah_R_-Haile-Aff2)[2](https://link.springer.com/article/10.1007/s15010-026-02768-0#Aff2),
- [Christian R. Kahlert](https://link.springer.com/article/10.1007/s15010-026-02768-0#auth-Christian_R_-Kahlert-Aff1-Aff9)[1](https://link.springer.com/article/10.1007/s15010-026-02768-0#Aff1),[9](https://link.springer.com/article/10.1007/s15010-026-02768-0#Aff9),
- [Matthias von Kietzell](https://link.springer.com/article/10.1007/s15010-026-02768-0#auth-Matthias-Kietzell-Aff4)[4](https://link.springer.com/article/10.1007/s15010-026-02768-0#Aff4),
- [Stefan P. Kuster](https://link.springer.com/article/10.1007/s15010-026-02768-0#auth-Stefan_P_-Kuster-Aff1)[1](https://link.springer.com/article/10.1007/s15010-026-02768-0#Aff1),
- [Markus Rütti](https://link.springer.com/article/10.1007/s15010-026-02768-0#auth-Markus-R_tti-Aff5)[5](https://link.springer.com/article/10.1007/s15010-026-02768-0#Aff5),
- [Matthias Schlegel](https://link.springer.com/article/10.1007/s15010-026-02768-0#auth-Matthias-Schlegel-Aff1)[1](https://link.springer.com/article/10.1007/s15010-026-02768-0#Aff1),
- [Carol Strahm](https://link.springer.com/article/10.1007/s15010-026-02768-0#auth-Carol-Strahm-Aff1)[1](https://link.springer.com/article/10.1007/s15010-026-02768-0#Aff1),
- [Reto Stocker](https://link.springer.com/article/10.1007/s15010-026-02768-0#auth-Reto-Stocker-Aff6-Aff13)[6](https://link.springer.com/article/10.1007/s15010-026-02768-0#Aff6),[13](https://link.springer.com/article/10.1007/s15010-026-02768-0#Aff13),
- [Danielle Vuichard-Gysin](https://link.springer.com/article/10.1007/s15010-026-02768-0#auth-Danielle-Vuichard_Gysin-Aff7-Aff8)[7](https://link.springer.com/article/10.1007/s15010-026-02768-0#Aff7),[8](https://link.springer.com/article/10.1007/s15010-026-02768-0#Aff8),
- [Lorenz Risch](https://link.springer.com/article/10.1007/s15010-026-02768-0#auth-Lorenz-Risch-Aff10-Aff11-Aff12)[10](https://link.springer.com/article/10.1007/s15010-026-02768-0#Aff10),[11](https://link.springer.com/article/10.1007/s15010-026-02768-0#Aff11),[12](https://link.springer.com/article/10.1007/s15010-026-02768-0#Aff12),
- [Milo A. Puhan](https://link.springer.com/article/10.1007/s15010-026-02768-0#auth-Milo_A_-Puhan-Aff2)[2](https://link.springer.com/article/10.1007/s15010-026-02768-0#Aff2),
- [Tamara Dörr](https://link.springer.com/article/10.1007/s15010-026-02768-0#auth-Tamara-D_rr-Aff1)[1](https://link.springer.com/article/10.1007/s15010-026-02768-0#Aff1) [na1](https://link.springer.com/article/10.1007/s15010-026-02768-0#na1) &
- [Philipp Kohler](https://link.springer.com/article/10.1007/s15010-026-02768-0#auth-Philipp-Kohler-Aff1-Aff2)
[ORCID: orcid.org/0000-0003-0427-8934](https://orcid.org/0000-0003-0427-8934)[1](https://link.springer.com/article/10.1007/s15010-026-02768-0#Aff1),[2](https://link.springer.com/article/10.1007/s15010-026-02768-0#Aff2) [na1](https://link.springer.com/article/10.1007/s15010-026-02768-0#na1)
- [on behalf of the SURPRISE+ cohort](https://link.springer.com/article/10.1007/s15010-026-02768-0#group-1)
Show authors
- 9 Altmetric
## Abstract
### Purpose
Post-Acute Sequelae of SARS-CoV-2 Infection (PASC), or long COVID (LC), remains a significant burden for public health, with limited long-term data. This study aimed to assess the prevalence and evolution of PASC symptoms after ancestral SARS-CoV-2 (aSCV2) infection in a longitudinal healthcare worker (HCW) cohort.
### Methods
A multicentre cohort study involving HCWs from 14 institutions was conducted in Switzerland. Infection status was based on self-reported positive swabs, with additional serology used to confirm uninfected controls. Baseline was defined as the first survey conducted in 2022 (median 18.5 months post-infection), with follow-up surveys every 6 months through November 2024. To identify PASC-specific symptoms, 24 chronic symptoms were compared between 456 aSCV2-infected and 571 uninfected participants using chi-square tests at baseline. In aSCV2-infected individuals reporting PASC-specific symptoms, symptom trajectories and subjective LC were analyzed across follow-up surveys. Functional limitations were assessed using the Post-COVID Functional Status (PCFS) scale.
### Results
Thirteen of 24 symptoms were more common in aSCV2-infected individuals, with fatigue (22.8%), loss of smell/taste (11.4%), and brain fog (8.3%) being most prevalent. At baseline, 186/456 (40.8%) infected participants reported ≥ 1 PASC-specific symptom. Most symptoms declined in prevalence up to the last survey (median 47.5 months post-infection), although 41/70 (58.6%) remaining participants still reported ≥ 1 PASC symptom. Subjective LC was reported by 70/186 (37.6%) and was associated with higher symptom burden. PCFS scores showed slight impairments in most cases, although moderate-to-severe limitations often persisted.
### Conclusions
PASC symptoms persisted up to four years after aSCV2 infection in a substantial proportion of HCWs.
### Similar content being viewed by others

### [Burden of post–acute COVID-19 sequelae in healthcare workers and its course over a 30-month period–results from a prospective multicentre cohort](https://link.springer.com/10.1007/s15010-024-02418-3)
Article Open access 12 November 2024

### [A longitudinal SARS-CoV-2 biorepository for COVID-19 survivors with and without post-acute sequelae](https://link.springer.com/10.1186/s12879-021-06359-2)
Article Open access 13 July 2021

### [Factors Associated with Post-Acute Sequelae of SARS-CoV-2 (PASC) After Diagnosis of Symptomatic COVID-19 in the Inpatient and Outpatient Setting in a Diverse Cohort](https://link.springer.com/10.1007/s11606-022-07523-3)
Article Open access 07 April 2022
## Introduction
Although acute SARS-CoV-2 infection has caused significant mortality and morbidity, attention has increasingly shifted to its long-term effects, commonly referred to as Post-Acute Sequelae of SARS-CoV-2 Infection (PASC) or long COVID (LC). PASC is defined as symptoms that persist or newly develop at least three months after acute infection, last for at least two months, and cannot be explained by alternative diagnoses \[[1](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR1 "Post COVID-19 condition (Long COVID) [Internet].
https://www.who.int/europe/news-room/fact-sheets/item/post-covid-19-condition
. Accessed 15 Jan 2025."), [2](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR2 "Parums DV. Long COVID or Post-Acute Sequelae of SARS-CoV-2 Infection (PASC) and the urgent need to identify diagnostic biomarkers and risk factors. Med Sci Monit. 2024.
https://doi.org/10.12659/MSM.946512
.")\]. It includes a wide range of symptoms affecting multiple organ systems, with fatigue, cognitive dysfunction, and respiratory symptoms being most common \[[3](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR3 "Davis HE, McCorkell L, Vogel JM, Topol EJ. Long COVID: major findings, mechanisms and recommendations. Nat Rev Microbiol. 2023;21:133–46.
https://doi.org/10.1038/s41579-022-00846-2
."),[4](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR4 "Reese JT, Blau H, Casiraghi E, Bergquist T, Loomba JJ, Callahan TJ, et al. Generalisable long COVID subtypes: findings from the NIH N3C and RECOVER programmes. EBioMedicine. 2023;87:104413.
https://doi.org/10.1016/j.ebiom.2022.104413
."),[5](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR5 "Thaweethai T, Jolley SE, Karlson EW, Levitan EB, Levy B, McComsey GA, et al. Development of a definition of postacute sequelae of SARS-CoV-2 infection. JAMA. 2023;329:1934.
https://doi.org/10.1001/jama.2023.8823
."),[6](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR6 "Griffin DO. Postacute sequelae of COVID (PASC or Long COVID): an evidenced-based approach. Open Forum Infect Dis. 2024;11:ofae462.
https://doi.org/10.1093/ofid/ofae462
."),[7](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR7 "Hastie CE, Lowe DJ, McAuley A, Mills NL, Winter AJ, Black C, et al. True prevalence of long-COVID in a nationwide, population cohort study. Nat Commun. 2023;14:7892.
https://doi.org/10.1038/s41467-023-43661-w
."),[8](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR8 "Xie Y, Choi T, Al-Aly Z. Postacute sequelae of SARS-CoV-2 infection in the Pre-Delta, Delta, and Omicron eras. N Engl J Med. 2024;391:515–25.
https://doi.org/10.1056/NEJMoa2403211
."),[9](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR9 "Sherif ZA, Gomez CR, Connors TJ, Henrich TJ, Reeves WB, RECOVER Mechanistic Pathway Task Force. Pathogenic mechanisms of post-acute sequelae of SARS-CoV-2 infection (PASC). Elife. 2023;12:e86002.
https://doi.org/10.7554/eLife.86002
.")\]. However, many of these symptoms also occur in non-infected individuals and are not specific for PASC. Additionally, not all individuals reporting PASC symptoms consider themselves to suffer from LC, highlighting the heterogeneity of post-COVID outcomes and the challenges of their assessment. Prevalence estimates of PASC vary across studies, ranging from 3 to 54%, depending on the PASC definition, population, sampling scheme, severity and time since initial infection, vaccination status, as well as the viral variant \[[5](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR5 "Thaweethai T, Jolley SE, Karlson EW, Levitan EB, Levy B, McComsey GA, et al. Development of a definition of postacute sequelae of SARS-CoV-2 infection. JAMA. 2023;329:1934.
https://doi.org/10.1001/jama.2023.8823
."), [8](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR8 "Xie Y, Choi T, Al-Aly Z. Postacute sequelae of SARS-CoV-2 infection in the Pre-Delta, Delta, and Omicron eras. N Engl J Med. 2024;391:515–25.
https://doi.org/10.1056/NEJMoa2403211
."), [10](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR10 "Mandel H, Yoo YJ, Allen AJ, Abedian S, Verzani Z, Karlson EW, et al. Long COVID incidence proportion in adults and children between 2020 and 2024: an EHR-based study from the RECOVER initiative. Clin Infect Dis. 2025.
https://doi.org/10.1093/cid/ciaf046
."),[11](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR11 "Cai M, Xie Y, Topol EJ, Al-Aly Z. Three-year outcomes of post-acute sequelae of COVID-19. Nat Med. 2024;30:1564–73.
https://doi.org/10.1038/s41591-024-02987-8
."),[12](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR12 "Groff D, Sun A, Ssentongo AE, Ba DM, Parsons N, Poudel GR, et al. Short-term and long-term rates of postacute sequelae of SARS-CoV-2 infection: a systematic review. JAMA Netw Open. 2021;4:e2128568.
https://doi.org/10.1001/jamanetworkopen.2021.28568
."),[13](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR13 "Kahlert CR, Strahm C, Güsewell S, Cusini A, Brucher A, Goppel S, et al. Post-acute sequelae after Severe Acute Respiratory Syndrome Coronavirus 2 infection by viral variant and vaccination status: a multicenter cross-sectional study. Clin Infect Dis. 2023;77:194–202.
https://doi.org/10.1093/cid/ciad143
."),[14](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR14 "Dörr T, Strahm C, Güsewell S, Ballouz T, Kocan E, Cusini A, et al. Burden of post–acute COVID-19 sequelae in healthcare workers and its course over a 30-month period–results from a prospective multicentre cohort. Infection. 2024.
https://doi.org/10.1007/s15010-024-02418-3
."),[15](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR15 "Ballouz T, Menges D, Anagnostopoulos A, Domenghino A, Aschmann HE, Frei A, et al. Recovery and symptom trajectories up to two years after SARS-CoV-2 infection: population based, longitudinal cohort study. BMJ. 2023;381:e074425.
https://doi.org/10.1136/bmj-2022-074425
. (British Medical Journal Publishing Group;).")\]. Comparative analyses show that the risk of developing PASC is highest after infection with ancestral SARS-CoV-2 (aSCV2) and decreases with subsequent variants \[[5](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR5 "Thaweethai T, Jolley SE, Karlson EW, Levitan EB, Levy B, McComsey GA, et al. Development of a definition of postacute sequelae of SARS-CoV-2 infection. JAMA. 2023;329:1934.
https://doi.org/10.1001/jama.2023.8823
."), [8](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR8 "Xie Y, Choi T, Al-Aly Z. Postacute sequelae of SARS-CoV-2 infection in the Pre-Delta, Delta, and Omicron eras. N Engl J Med. 2024;391:515–25.
https://doi.org/10.1056/NEJMoa2403211
."), [13](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR13 "Kahlert CR, Strahm C, Güsewell S, Cusini A, Brucher A, Goppel S, et al. Post-acute sequelae after Severe Acute Respiratory Syndrome Coronavirus 2 infection by viral variant and vaccination status: a multicenter cross-sectional study. Clin Infect Dis. 2023;77:194–202.
https://doi.org/10.1093/cid/ciad143
.")\].
During the aSCV2-dominant period of the pandemic, health care workers (HCWs) were particularly affected by PASC due to their increased exposure to SARS-CoV-2, with prevalence rates noticeably higher than those observed in the general population \[[13](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR13 "Kahlert CR, Strahm C, Güsewell S, Cusini A, Brucher A, Goppel S, et al. Post-acute sequelae after Severe Acute Respiratory Syndrome Coronavirus 2 infection by viral variant and vaccination status: a multicenter cross-sectional study. Clin Infect Dis. 2023;77:194–202.
https://doi.org/10.1093/cid/ciad143
."), [14](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR14 "Dörr T, Strahm C, Güsewell S, Ballouz T, Kocan E, Cusini A, et al. Burden of post–acute COVID-19 sequelae in healthcare workers and its course over a 30-month period–results from a prospective multicentre cohort. Infection. 2024.
https://doi.org/10.1007/s15010-024-02418-3
."), [16](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR16 "Foulkes S, Evans J, Neill C, Bishop J, Khawam J, Islam J, et al. Prevalence and impact of persistent symptoms following SARS-CoV-2 infection among healthcare workers: a cross-sectional survey in the SIREN cohort. J Infect. 2024;89:106259.
https://doi.org/10.1016/j.jinf.2024.106259
."),[17](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR17 "Lim SH, Lim YC, Zaki RA, Johari BM, Chang CY, Omar SFS, et al. Prevalence and predictors of post-acute COVID syndrome among infected healthcare workers at University Malaya Medical Centre. PLoS ONE. 2024;19:e0298376.
https://doi.org/10.1371/journal.pone.0298376
."),[18](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR18 "Dempsey B, Blake HA, Madan I, Stevelink SAM, Greenberg N, Raine R, et al. Post COVID-19 syndrome among 5248 healthcare workers in England: longitudinal findings from NHS CHECK. Occup Environ Med. 2024;81:471–9.
https://doi.org/10.1136/oemed-2024-109621
.")\]. Analysis of PASC trajectories in the general population showed a decline in prevalence, especially during the first year after infection \[[15](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR15 "Ballouz T, Menges D, Anagnostopoulos A, Domenghino A, Aschmann HE, Frei A, et al. Recovery and symptom trajectories up to two years after SARS-CoV-2 infection: population based, longitudinal cohort study. BMJ. 2023;381:e074425.
https://doi.org/10.1136/bmj-2022-074425
. (British Medical Journal Publishing Group;)."), [19](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR19 "Bowe B, Xie Y, Al-Aly Z. Postacute sequelae of COVID-19 at 2 years. Nat Med. 2023;29:2347–57.
https://doi.org/10.1038/s41591-023-02521-2
."), [20](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR20 "Hurme A, Viinanen A, Teräsjärvi J, Jalkanen P, Feuth T, Löyttyniemi E, et al. Post-COVID-19 condition in prospective inpatient and outpatient cohorts. Sci Rep. 2025;15:6925.
https://doi.org/10.1038/s41598-025-90819-1
.")\]. Nevertheless, a substantial proportion of individuals (18–47%) continued to experience PASC symptoms two years post-infection \[[15](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR15 "Ballouz T, Menges D, Anagnostopoulos A, Domenghino A, Aschmann HE, Frei A, et al. Recovery and symptom trajectories up to two years after SARS-CoV-2 infection: population based, longitudinal cohort study. BMJ. 2023;381:e074425.
https://doi.org/10.1136/bmj-2022-074425
. (British Medical Journal Publishing Group;)."), [20](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR20 "Hurme A, Viinanen A, Teräsjärvi J, Jalkanen P, Feuth T, Löyttyniemi E, et al. Post-COVID-19 condition in prospective inpatient and outpatient cohorts. Sci Rep. 2025;15:6925.
https://doi.org/10.1038/s41598-025-90819-1
."), [21](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR21 "Pfrommer LR, Diexer S, Klee B, Massag J, Gottschick C, Purschke O, et al. Post-COVID recovery is faster after an infection with the SARS-CoV-2 Omicron variant: a population-based cohort study. Infection. 2025;53:657–65.
https://doi.org/10.1007/s15010-024-02438-z
.")\]. Thereafter, available data is limited, especially among HCWs, although recent studies indicate a relevant ongoing burden of disease \[[11](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR11 "Cai M, Xie Y, Topol EJ, Al-Aly Z. Three-year outcomes of post-acute sequelae of COVID-19. Nat Med. 2024;30:1564–73.
https://doi.org/10.1038/s41591-024-02987-8
."), [22](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR22 "Rahmati M, Udeh R, Kang J, Dolja‐Gore X, McEvoy M, Kazemi A, et al. Long‐term sequelae of COVID‐19: a systematic review and meta‐analysis of symptoms 3 years post‐SARS‐CoV‐2 infection. J Med Virol. 2025;97:e70429.
https://doi.org/10.1002/jmv.70429
."),[23](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR23 "Vallée G, Xi D, Avramovic G, O’Kelly B, Lambert JS. Evaluating the longitudinal physical and psychological health effects of persistent long Covid 3.5 years after infection. PLoS ONE. 2025;20:e0326790.
https://doi.org/10.1371/journal.pone.0326790
."),[24](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR24 "Gottlieb M, Yu H, Chen J, Spatz ES, Gentile NL, Geyer RE, et al. Differences in Long COVID severity by duration of illness, symptom evolution, and vaccination: a longitudinal cohort study from the INSPIRE group. Lancet Reg Health Am. 2025;44:101026.
https://doi.org/10.1016/j.lana.2025.101026
."),[25](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR25 "Ballouz T, Kerksieck P, Haile SR, Dressel H, Hämmig O, Bauer GF, et al. Work ability trajectories and sick leave in individuals with post COVID-19 condition: 3-year follow-up of a population-based cohort. Lancet Reg Health Eur. 2026;61:101536.
https://doi.org/10.1016/j.lanepe.2025.101536
.")\].
To guide post-COVID-19 care and occupational health strategies, this study aims to identify PASC-specific symptoms and to investigate the evolution of PASC symptoms in HCWs up to four years after aSCV2 infection. We also compare individuals with and without subjective LC in terms of PASC symptomatology and assess changes in subjective LC and the associated limitations in daily living over time, for a more comprehensive understanding of both the clinical and self-perceived long-term impact of COVID-19.
## Methods
### Setting and participants
In 2022, a longitudinal multicentre cohort involving HCWs from 14 institutions in northeastern Switzerland was launched. Employees aged ≥ 16 years of any work type, with or without direct patient contact, were eligible for inclusion and all participants provided electronic informed consent. The study protocol was approved by the Ethics Committee of Eastern Switzerland (\#2020–00502).
### Data collection
#### Serological testing
Serological testing for anti-spike (anti-S) and anti-nucleocapsid (anti-N) antibodies was performed in May/June 2022 in all participants to identify asymptomatic infections \[[26](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR26 "Kahlert CR, Persi R, Güsewell S, Egger T, Leal-Neto OB, Sumer J, et al. Non-occupational and occupational factors associated with specific SARS-CoV-2 antibodies among hospital workers – a multicentre cross-sectional study. Clin Microbiol Infect. 2021;27:1336–44.
https://doi.org/10.1016/j.cmi.2021.05.014
.")\]. The antibodies were measured using the Roche Elecsys electrochemiluminescence immunoassay (Roche Diagnostics, Rotkreuz, Switzerland).
#### Baseline survey
At baseline (September 2022), data were collected through an electronic baseline questionnaire including questions on personal health, occupational and non-occupational exposures, SARS-CoV-2 infection and vaccination history.
#### Follow-up surveys
Follow-up surveys were conducted approximately every 6 months (March to April 2023, October to November 2023, April to May 2024, October to November 2024). In those questionnaires, participants indicated the presence and duration of PASC-compatible symptoms as well as whether they suffer from LC (ongoing, resolved, never experienced). Additionally, SARS-CoV-2 infection and vaccination status were regularly updated.
### Definitions
#### Infection status
Participants were classified as aSCV2-infected if they reported a positive SARS-CoV-2 swab between February 2020 and January 2021 \[[27](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR27 "Federal Office of Public Health. Virus variants overview. [Internet]. [cited 2025 Apr 21].
https://www.covid19.admin.ch/en/epidemiologic/virus-variants
. Accessed 21 Apr 2025.")\]. Participants were assigned to the uninfected control group if they reported no previous SARS-CoV-2 infection and had a negative anti-N antibody result in June 2022. Thus, participants with a positive swab after January 2021 or positive anti-N antibody results in June 2022 were excluded, ensuring that only aSCV2-infected and uninfected participants were included, while individuals infected with later viral variants were not considered. Potential reinfections after the initial aSCV2 infection were not considered, as testing for SARS-CoV-2 was no longer recommended by the Swiss Federal Office of Public Health after February 2022, leading to incomplete detection of later infections \[[28](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR28 "Coronavirus: Key Decisions of the Federal Council [Internet]. [cited 2025 May 2].
https://www.uvek.admin.ch/uvek/de/home/uvek/coronavirus/wichtige-entscheide.html
. Accessed 2 May 2025.")\]. Validation of self-reported swab results with data from the division of occupational medicine (performed in the largest participating hospital) showed excellent concordance \[[29](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR29 "Kohler P, Güsewell S, Seneghini M, Egger T, Leal O, Brucher A, et al. Impact of baseline SARS-CoV-2 antibody status on syndromic surveillance and the risk of subsequent COVID-19—a prospective multicenter cohort study. BMC Med. 2021;19:270.
https://doi.org/10.1186/s12916-021-02144-9
.")\].
#### PASC symptoms
The 24 symptoms included in the surveys were selected based on national SARS-CoV-2 testing recommendations during the early phase of the pandemic. The symptoms were: Fatigue, Loss of Smell/Taste, Brain Fog, Joint Pain, Hair Loss, Headache, Chest Pain, Muscle Pain, Shortness of Breath, Dizziness, Cough, Burnout or Exhaustion, Runny Nose, Fever, Sneezing, Sore Throat, Abdominal Pain, Loss of Appetite/Nausea, Chills or Shivering, Red or Itchy Eyes, Erectile Dysfunction, Diarrhea, Menstrual Complaints and Rash. Testing for SARS-CoV-2 in individuals with compatible symptoms, using either rapid antigen tests or polymerase chain reaction, was recommended and later became mandatory for access to public institutions, including hospitals, in Switzerland. Symptoms that were described as chronic (i.e., longer than 7 days) and had emerged after the start of the COVID-19 pandemic were considered as PASC-related. Indications of symptoms that were either acute or chronic with onset before the pandemic were assigned as being non-PASC-compatible.
#### Subjective LC and functional limitations
Subjective LC was based on participants’ self-assessment; no further diagnostic criteria were applied. Those self-reporting LC were asked to grade their attributed functional limitations using the PCFS, a scale used to assess the needs for rehabilitation or recovery in COVID-19 patients. It differentiates: 0 = no functional limitations, 1 = symptoms without significant impact on daily life, 2 = slight limitations of usual activities, 3 = substantial restrictions with reduced everyday functioning, and 4 = severe limitations with dependence on assistance for activities of daily living \[[30](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR30 "Klok FA, Boon GJAM, Barco S, Endres M, Geelhoed JJM, Knauss S, et al. The Post-COVID-19 Functional Status scale: a tool to measure functional status over time after COVID-19. Eur Respir J. 2020;56:2001494.
https://doi.org/10.1183/13993003.01494-2020
.")\].
### Study design
The study design entailed a cross-sectional and a longitudinal analysis. In the cross-sectional analysis, PASC-specific symptoms were identified by comparing aSCV2-infected and uninfected individuals. In the longitudinal analysis, trajectories of symptoms, LC and PCFS were analyzed in aSCV2-infected participants that reported at least one PASC symptom at baseline (Fig. [1](https://link.springer.com/article/10.1007/s15010-026-02768-0#Fig1)).
**Fig. 1**
[](https://link.springer.com/article/10.1007/s15010-026-02768-0/figures/1)
Study Flow showing the process of enrolment and allocation to the different groups. N = Number of Participants, HCWs = Health Care Workers, LC = long COVID, PASC = Post-Acute COVID-19 Sequelae, aSCV2 = ancestral SARS-CoV-2
[Full size image](https://link.springer.com/article/10.1007/s15010-026-02768-0/figures/1)
### Statistical analysis
For the cross-sectional analysis, demographic and clinical characteristics between aSCV2-infected participants and the uninfected controls were compared using descriptive statistics. We calculated p-values using the Wilcoxon rank-sum test for continuous variables and the chi-square test or Fisher’s exact test for categorical variables. To distinguish PASC-specific symptoms from non-specific symptoms, the chi-square test was used; symptoms being significantly more common in the aSCV2 group were considered PASC-specific. Furthermore, baseline characteristics, symptom counts, and symptom prevalence were compared between participants with and without subjective LC using the same methods as described for aSCV2- and uninfected participants.
For the longitudinal analysis, we calculated the prevalence (for binary outcomes) and the median (for continuous outcomes) at every time point. Alluvial plots were used, where appropriate, to visualize how individuals move across categories over time. The independent effect of time on the number of symptoms and on the prevalence of the three most common symptoms (fatigue, brain fog and loss of smell/taste) was assessed using negative binomial (for symptom count) and logistic regression analysis (for symptoms). Time points were included as categorical and not as a continuous variable, as the effect of time was assumed to be non-linear. To account for repeated measurements, mixed-effects models with a random intercept for each individual were used. Adjusted incidence rate ratios (aIRR) from the negative binomial regression and adjusted odds ratios (aOR) from the logistic regression for the different time points, along with corresponding 95% confidence intervals (CI) were calculated. The models were adjusted for a priori defined covariates, namely age, sex, and Body-Mass-Index (BMI). To account for attrition bias, sensitivity analyses were performed: one restricted to participants with complete data across all surveys and another by adding the number of observed time points per participant to the negative binomial regression model. Spearman’s rank correlation was used to assess the association between baseline and last follow-up values of PCFS and total symptom count.
Statistical significance was set at a p-value of \< 0.05. All statistical analyses and figures were created using R version 4.4.2 (2024–10-31); descriptive statistics were performed using “gtsummary”, for regression analyses the package “lme4” was used and correlation analyses were carried out using Base R.
## Results
### Study population
Of 3,986 HCWs who completed the survey in September 2022, 1,027 (25.8%) were included in the baseline analysis (median age: 44 years; 80.6% women), of whom 456 (44.4%) were aSCV2-infected and 571 (55.6%) were uninfected controls. A total of 2,959 participants were excluded due to infections during later pandemic phases or incomplete baseline surveys (Fig. [1](https://link.springer.com/article/10.1007/s15010-026-02768-0#Fig1); Supplementary Material Table S1).
Compared to controls, aSCV2-infected participants were younger (median age 41 vs. 47 years, p \< 0.001), more frequently employed as nurses (59.4% vs. 37.5%, p \< 0.001) and had children under age 6 at home (13.6% vs. 9.3%, p = 0.029), while a smaller proportion were smokers (13.6% vs. 21.4%, p = 0.001) (Table [1](https://link.springer.com/article/10.1007/s15010-026-02768-0#Tab1)). The median time from the first positive SARS-CoV-2 test to the baseline survey was 18.5 months and 47.5 months to the last survey (Supplementary Material Table S2).
**Table 1 Characteristics of the aSCV2-Infected Group Compared with the Non-Infected Control Group at Baseline (09/2022)**
[Full size table](https://link.springer.com/article/10.1007/s15010-026-02768-0/tables/1)
### Identification of PASC-specific symptoms and subjective LC
Among 24 potential PASC symptoms, 13 symptoms were significantly more common in the aSCV2 group, with fatigue (22.8% in aSCV2-infected and 7.4% in controls), loss of smell/taste (11.4% and 0.4%), and brain fog (8.3% and 1.8%) being the most frequent (Fig. [2](https://link.springer.com/article/10.1007/s15010-026-02768-0#Fig2); Supplementary Material Table S3).
**Fig. 2**
[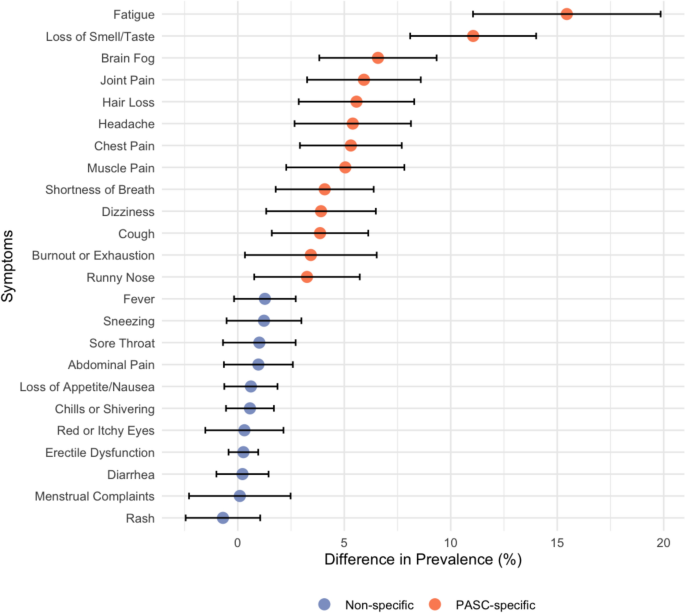](https://link.springer.com/article/10.1007/s15010-026-02768-0/figures/2)
Absolute difference in symptom prevalence (%) between the ancestral SARS CoV-2 (aSCV2) infected group and the non-infected control group at baseline (09/2022) represented as dots, with 95% confidence intervals. Orange = PASC-specific symptoms; blue = non-specific symptoms
[Full size image](https://link.springer.com/article/10.1007/s15010-026-02768-0/figures/2)
Among HCWs with PASC-specific symptoms at baseline (n = 186/1027, 18.1%), 38% (n = 70) self-reported having LC, while 62% (n = 116) did not (anymore). Participants with subjective LC at baseline had a higher median number of symptoms compared to those without subjective LC (4 vs 1) (Table S4).
### Trajectory of symptoms
Out of 456 aSCV2-infected participants, 40.8% (n = 186) reported at least one PASC-specific symptom and were included in the longitudinal analysis. Participants completed a median of 3 surveys (range 1–5). Overall, 72.0% (n = 134) did not have complete data or were lost to follow-up during the course of the study. Compared to those with complete data, these participants were younger (median age 39 vs. 47.5 years), more often male (14.9% vs. 23.1%), more commonly smokers (11.9% vs. 5.8%) and more frequently working full-time (45.5% vs. 34.6%). Additionally, they were less likely to report comorbidities other than pollen allergy (33.3% vs. 58.6%) (Supplementary Material Table S5).
The median number of symptoms declined from 2 at baseline to 0 symptoms in the last survey, and from 2 to 1 in participants with complete data (n = 52); the decline was most pronounced from the baseline to the first follow-up survey and remained mostly stable thereafter (Fig. [3](https://link.springer.com/article/10.1007/s15010-026-02768-0#Fig3); Supplementary Material Table S6). In the last survey (median 47.5 months after infection), 58.6% of all participants (59.6% of participants with complete data) still reported ≥ 1 PASC symptom, with fatigue being the most persistent symptom (35.7%) (Supplementary Material Table S7/ Table S8). For those with complete data, participants with an initially high number of symptoms tended to also have higher symptom scores in the last survey (Spearman’s ρ = 0.338, p = 0.014) (Fig. [3](https://link.springer.com/article/10.1007/s15010-026-02768-0#Fig3); Supplementary Material Figure S1).
**Fig. 3**
[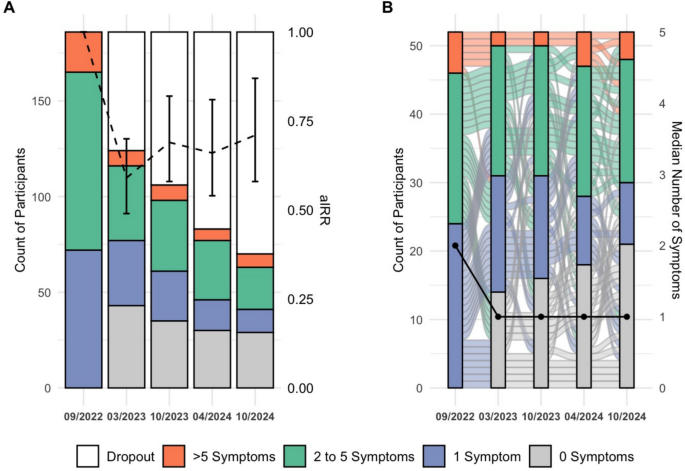](https://link.springer.com/article/10.1007/s15010-026-02768-0/figures/3)
**A** displays the count of symptoms for each time point, grouped as described in the legend, for all participants including participants that dropped out (n=186). The dashed black line and error bars represent the adjusted incidence rate ratio (aIRR) and 95% confidence intervals for symptom count, referenced to baseline (09/2022). **B** shows longitudinal trajectories of symptom groups among participants with complete data at every time point (n=52), with the black solid line indicating the median number of symptoms at each time point
[Full size image](https://link.springer.com/article/10.1007/s15010-026-02768-0/figures/3)
Assessment of symptom trajectories using the negative binomial mixed-effects model showed a significant decline in the number of symptoms per participant at the last survey compared to baseline (aIRR 0.71, 95% CI 0.58–0.87, p = 0.001). Results were similar with complete case analysis (aIRR = 0.72, 95% CI 0.56–0.93, p = 0.013) (Supplementary Material Table S9).
For the three most prevalent symptoms, fatigue decreased from 55.9% (104/186) to 35.7% (25/70) (aOR 0.23, 95% CI 0.10–0.52, p \< 0.001), loss of smell/taste from 28.0% (52/186) to 18.6% (13/70) (aOR 0.03, 95% CI 0.00–0.21, p \< 0.001) and brain fog changed from 20.4% (38/186) to 14.3% (10/70) without being significant (aOR 0.96, 95% CI 0.27–3.37, p = 0.95) (Fig. [4](https://link.springer.com/article/10.1007/s15010-026-02768-0#Fig4)). Figures were similar in the subset of participants with complete data (Supplementary Material Figure S2; Table S10).
**Fig. 4**
[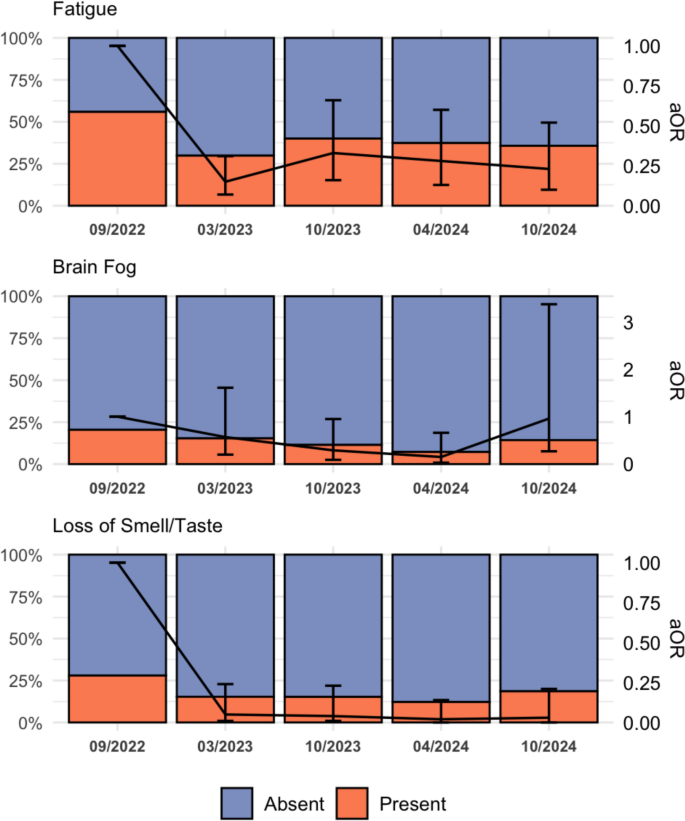](https://link.springer.com/article/10.1007/s15010-026-02768-0/figures/4)
Bar graphs showing the prevalence of the three most prevalent PASC-specific symptoms (Fatigue, Brain Fog, Loss of Smell/ Taste) in participants with available data at each follow-up time point. The black line shows the adjusted Odds Ratio (aOR) with 95% confidence intervals for symptom presence at each time point (relative to baseline), shown as error bars. Sample size: 09/2022: n=186, 03/2023: n=124, 10/2023: n=105, 04/2024: n=83, 10/2024: n=70
[Full size image](https://link.springer.com/article/10.1007/s15010-026-02768-0/figures/4)
### Trajectory of subjective LC and functional status
77 of the 456 aSCV2-infected participants reported LC at baseline. To ensure consistency with the longitudinal symptom trajectory analyses, only participants reporting ≥ 1 PASC-specific chronic symptom were included. In this subgroup, 70 of 186 individuals reported subjective LC, of whom 12.9% (9/70) reported resolution of symptoms at the first follow-up. Thereafter, there were no new reports of resolved symptoms. At the final follow-up, only 18 of the initial 70 participants remained, with 14 indicating ongoing subjective LC (Supplementary Material Figure S3; Table S11).
When analyzing the PCFS score at baseline, 71.4% (n = 50) of participants with subjective LC had no or minor (PCFS 0 or 1) limitations in their daily life. This figure remained stable over time as did the median PCFS. Participants with moderate or severe limitations (PCFS score ≥ 2) at baseline tended to still report limitations at the final follow-up (Spearman’s ρ = 0.40, p = 0.10). However, data availability declined over follow-up due to decreasing subjective LC reports and participant attrition (Supplementary Material Figures S4, S5; Table S12).
## Discussion
In a prospective multicentre cohort of HCWs, we demonstrate a non-linear decline in PASC-specific symptoms over time, with up to 60% of individuals still reporting symptoms after a median of almost 4 years after aSCV2 infection. Fatigue, brain fog, and loss of smell or taste are the most prevalent symptoms. For those with subjective LC, the limitations in daily life are mostly mild, but often persist over time.
The prevalence of PASC symptoms at baseline was 40.8% (median 18.5 months post-infection), which is higher than reported in prior studies \[[15](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR15 "Ballouz T, Menges D, Anagnostopoulos A, Domenghino A, Aschmann HE, Frei A, et al. Recovery and symptom trajectories up to two years after SARS-CoV-2 infection: population based, longitudinal cohort study. BMJ. 2023;381:e074425.
https://doi.org/10.1136/bmj-2022-074425
. (British Medical Journal Publishing Group;)."), [31](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR31 "Fernandez-de-las-Peñas C, Notarte KI, Macasaet R, Velasco JV, Catahay JA, Ver AT, et al. Persistence of post-COVID symptoms in the general population two years after SARS-CoV-2 infection: a systematic review and meta-analysis. J Infect. 2024;88:77–88.
https://doi.org/10.1016/j.jinf.2023.12.004
."), [32](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR32 "Kim Y, Bae S, Chang H-H, Kim S-W. Long COVID prevalence and impact on quality of life 2 years after acute COVID-19. Sci Rep. 2023;13:11207.
https://doi.org/10.1038/s41598-023-36995-4
.")\]. A recent meta-analysis including only studies with more than 3 years of follow-up, showed a pooled prevalence of 20% at 3 years, again lower than our findings (67% at 3 years). However, the individual studies contributing to this analysis showed a wide range of prevalence estimates (6–54%) \[[22](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR22 "Rahmati M, Udeh R, Kang J, Dolja‐Gore X, McEvoy M, Kazemi A, et al. Long‐term sequelae of COVID‐19: a systematic review and meta‐analysis of symptoms 3 years post‐SARS‐CoV‐2 infection. J Med Virol. 2025;97:e70429.
https://doi.org/10.1002/jmv.70429
.")\]. One factor for this difference could be the high exposure of our cohort during the aSCV2 period compared to non-HCWs, as this viral variant was shown to have the highest PASC incidence one year post-infection, with declining rates observed for later variants \[[8](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR8 "Xie Y, Choi T, Al-Aly Z. Postacute sequelae of SARS-CoV-2 infection in the Pre-Delta, Delta, and Omicron eras. N Engl J Med. 2024;391:515–25.
https://doi.org/10.1056/NEJMoa2403211
.")\]. Consistent with previous reports of neurological symptoms persisting, brain fog showed no significant decline, suggesting ongoing cognitive impairment in PASC affected patients \[[15](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR15 "Ballouz T, Menges D, Anagnostopoulos A, Domenghino A, Aschmann HE, Frei A, et al. Recovery and symptom trajectories up to two years after SARS-CoV-2 infection: population based, longitudinal cohort study. BMJ. 2023;381:e074425.
https://doi.org/10.1136/bmj-2022-074425
. (British Medical Journal Publishing Group;)."), [33](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR33 "Nguyen NN, Tissot-Dupont H, Brouqui P, Gautret P. Post-COVID syndrome in symptomatic COVID-19 patients: a retrospective cohort study. BMC Infect Dis. 2025;25:1099.
https://doi.org/10.1186/s12879-025-11360-0
.")\].
In our cohort, self-reported LC was associated with a higher number of symptoms and specific symptoms, most notably fatigue (80% vs. 41% without LC), which is in line with previous findings \[[34](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR34 "Danesh V, Arroliga AC, Bourgeois JA, Boehm LM, McNeal MJ, Widmer AJ, et al. Symptom clusters seen in adult COVID-19 recovery clinic care seekers. J Gen Intern Med. 2023;38:442–9.
https://doi.org/10.1007/s11606-022-07908-4
."),[35](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR35 "Huiberts AJ, De Bruijn S, Andeweg SP, Hoeve CE, Schipper M, De Melker HE, et al. Prospective cohort study of fatigue before and after SARS-CoV-2 infection in the Netherlands. Nat Commun. 2025;16:1923.
https://doi.org/10.1038/s41467-025-56994-5
."),[36](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR36 "Strahm C, Seneghini M, Güsewell S, Egger T, Leal-Neto O, Brucher A, et al. Symptoms compatible with long coronavirus disease (COVID) in healthcare workers with and without severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection—results of a prospective multicenter cohort. Clin Infect Dis. 2022;75:e1011–9.
https://doi.org/10.1093/cid/ciac054
.")\]. Gottlieb et al. had a similar design with self-reported LC through continuous surveys. In a cross-sectional analysis up to 40 months post-infection, only 2% reported resolved LC and only 26% of participants with current LC reported improved symptoms \[[24](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR24 "Gottlieb M, Yu H, Chen J, Spatz ES, Gentile NL, Geyer RE, et al. Differences in Long COVID severity by duration of illness, symptom evolution, and vaccination: a longitudinal cohort study from the INSPIRE group. Lancet Reg Health Am. 2025;44:101026.
https://doi.org/10.1016/j.lana.2025.101026
.")\]. This persistence of LC is consistent with our analysis of subjective LC prevalence, where no participants reported resolved symptoms after the first follow-up and the trend in functional limitations (PCFS), where only a small subset reported complete resolution of limitations.
Our findings indicate that full recovery from PASC remains uncertain for many patients and functional limitations persist. PASC should be recognized as a chronic condition requiring long-term clinical and social support, and further research has to be supported to clarify the pathophysiology and to identify diagnostic markers and effective treatment. As our cohort consists of HCWs, these findings underline the need for occupational health strategies, including structured return-to-work programs and flexible workload adjustments, to support sustainable reintegration and minimize the loss of essential workforce.
### Limitations
This study has several limitations. First, prior infection status was partially based on anti-N antibody negativity. We acknowledge that some previously infected individuals may have been misclassified due to absent seroconversion or declining antibody levels over time, which may have led to misclassification in the cross-sectional analysis and to over- or underestimation of symptom prevalence across time points \[[37](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR37 "Nakagama Y, Komase Y, Kaku N, Nitahara Y, Tshibangu-Kabamba E, Tominaga T, et al. Detecting waning serological response with commercial immunoassays: 18-month longitudinal follow-up of anti-SARS-CoV-2 Nucleocapsid antibodies. Microbiol Spectr. 2022;10:e00986-22.
https://doi.org/10.1128/spectrum.00986-22
.")\]. To minimize this risk, we not only required anti-N negativity for classification into the uninfected control group, but also the absence of a documented positive SARS-CoV-2 test. Given the extensive and partly mandatory testing policies for HCWs until February 2022, we consider the likelihood of undetected infections in our cohort to be low.
Second, information bias due to self-reported data may have caused misclassification and over- or underestimation of prevalence rates.
Third, substantial loss to follow-up limited the size of the dataset and potentially introduced attrition bias, causing an underestimation of PASC-prevalence if affected participants were less likely to remain in the study. However, sensitivity analyses focusing on participants with complete data and a model adjusted for the number of answered surveys mostly confirmed our results. Although regression models were adjusted for age, sex, and BMI, residual confounding by unmeasured factors, such as pre-existing comorbidities, mental health status, or occupational stress is possible. These factors may have influenced both the likelihood of infection and the reporting of persistent symptoms, potentially leading to over- or underestimation of the observed outcomes. In addition, effect modification by baseline health status or pre-existing comorbidities cannot be ruled out.
Fourth, survivor bias cannot be excluded. Only individuals who survived aSCV2 infection and remained in the workforce until 2022 were eligible for inclusion. Individuals who experienced severe outcomes, left the workforce due to functional impairment, or died were not captured, which may have led to an underestimation of the true long-term burden of PASC.
Fifth, reinfections were not assessed, as mandatory SARS-CoV-2 testing in Switzerland was discontinued in February 2022; undetected reinfections may therefore have biased symptom trajectories \[[28](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR28 "Coronavirus: Key Decisions of the Federal Council [Internet]. [cited 2025 May 2].
https://www.uvek.admin.ch/uvek/de/home/uvek/coronavirus/wichtige-entscheide.html
. Accessed 2 May 2025.")\].
Finally, the transferability of our findings to the general population is limited, as HCWs may differ in exposure risk and health-seeking behavior.
Strengths of this study include clearly defined infection groups through serology and timing, and a unique follow-up period providing data up to four years post-infection. Furthermore, PCFS scoring allowed assessment of functional limitations over time.
This study provides four-year follow-up data on PASC in a predominantly young and healthy cohort. Despite a general decline in symptom prevalence, key symptoms such as fatigue, brain fog, and loss of smell or taste persisted in a substantial subset up to four years post-aSCV2 infection. Long-term follow-up and tailored care strategies appear essential for managing persistent PASC symptoms.
## Data availability
All data generated or analysed during this study are included in this published article and its Supplementary Material.
## References
1. Post COVID-19 condition (Long COVID) \[Internet\]. <https://www.who.int/europe/news-room/fact-sheets/item/post-covid-19-condition>. Accessed 15 Jan 2025.
2. Parums DV. Long COVID or Post-Acute Sequelae of SARS-CoV-2 Infection (PASC) and the urgent need to identify diagnostic biomarkers and risk factors. Med Sci Monit. 2024. <https://doi.org/10.12659/MSM.946512>.
[Article](https://doi.org/10.12659%2FMSM.946512) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=39616449) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC11619173) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Long%20COVID%20or%20Post-Acute%20Sequelae%20of%20SARS-CoV-2%20Infection%20%28PASC%29%20and%20the%20urgent%20need%20to%20identify%20diagnostic%20biomarkers%20and%20risk%20factors&journal=Med%20Sci%20Monit&doi=10.12659%2FMSM.946512&publication_year=2024&author=Parums%2CDV)
3. Davis HE, McCorkell L, Vogel JM, Topol EJ. Long COVID: major findings, mechanisms and recommendations. Nat Rev Microbiol. 2023;21:133–46. <https://doi.org/10.1038/s41579-022-00846-2>.
[Article](https://doi.org/10.1038%2Fs41579-022-00846-2) [CAS](https://link.springer.com/articles/cas-redirect/1:CAS:528:DC%2BB3sXhtV2rtrw%3D) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=36639608) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC9839201) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Long%20COVID%3A%20major%20findings%2C%20mechanisms%20and%20recommendations&journal=Nat%20Rev%20Microbiol&doi=10.1038%2Fs41579-022-00846-2&volume=21&pages=133-146&publication_year=2023&author=Davis%2CHE&author=McCorkell%2CL&author=Vogel%2CJM&author=Topol%2CEJ)
4. Reese JT, Blau H, Casiraghi E, Bergquist T, Loomba JJ, Callahan TJ, et al. Generalisable long COVID subtypes: findings from the NIH N3C and RECOVER programmes. EBioMedicine. 2023;87:104413. <https://doi.org/10.1016/j.ebiom.2022.104413>.
[Article](https://doi.org/10.1016%2Fj.ebiom.2022.104413) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=36563487) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Generalisable%20long%20COVID%20subtypes%3A%20findings%20from%20the%20NIH%20N3C%20and%20RECOVER%20programmes&journal=EBioMedicine&doi=10.1016%2Fj.ebiom.2022.104413&volume=87&publication_year=2023&author=Reese%2CJT&author=Blau%2CH&author=Casiraghi%2CE&author=Bergquist%2CT&author=Loomba%2CJJ&author=Callahan%2CTJ)
5. Thaweethai T, Jolley SE, Karlson EW, Levitan EB, Levy B, McComsey GA, et al. Development of a definition of postacute sequelae of SARS-CoV-2 infection. JAMA. 2023;329:1934. <https://doi.org/10.1001/jama.2023.8823>.
[Article](https://doi.org/10.1001%2Fjama.2023.8823) [CAS](https://link.springer.com/articles/cas-redirect/1:CAS:528:DC%2BB3sXht1KqtL%2FL) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=37278994) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC10214179) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Development%20of%20a%20definition%20of%20postacute%20sequelae%20of%20SARS-CoV-2%20infection&journal=JAMA&doi=10.1001%2Fjama.2023.8823&volume=329&publication_year=2023&author=Thaweethai%2CT&author=Jolley%2CSE&author=Karlson%2CEW&author=Levitan%2CEB&author=Levy%2CB&author=McComsey%2CGA)
6. Griffin DO. Postacute sequelae of COVID (PASC or Long COVID): an evidenced-based approach. Open Forum Infect Dis. 2024;11:ofae462. <https://doi.org/10.1093/ofid/ofae462>.
[Article](https://doi.org/10.1093%2Fofid%2Fofae462) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=39220656) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC11363684) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Postacute%20sequelae%20of%20COVID%20%28PASC%20or%20Long%20COVID%29%3A%20an%20evidenced-based%20approach&journal=Open%20Forum%20Infect%20Dis&doi=10.1093%2Fofid%2Fofae462&volume=11&publication_year=2024&author=Griffin%2CDO)
7. Hastie CE, Lowe DJ, McAuley A, Mills NL, Winter AJ, Black C, et al. True prevalence of long-COVID in a nationwide, population cohort study. Nat Commun. 2023;14:7892. <https://doi.org/10.1038/s41467-023-43661-w>.
[Article](https://doi.org/10.1038%2Fs41467-023-43661-w) [CAS](https://link.springer.com/articles/cas-redirect/1:CAS:528:DC%2BB3sXisFSls7rP) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=38036541) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC10689486) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=True%20prevalence%20of%20long-COVID%20in%20a%20nationwide%2C%20population%20cohort%20study&journal=Nat%20Commun&doi=10.1038%2Fs41467-023-43661-w&volume=14&publication_year=2023&author=Hastie%2CCE&author=Lowe%2CDJ&author=McAuley%2CA&author=Mills%2CNL&author=Winter%2CAJ&author=Black%2CC)
8. Xie Y, Choi T, Al-Aly Z. Postacute sequelae of SARS-CoV-2 infection in the Pre-Delta, Delta, and Omicron eras. N Engl J Med. 2024;391:515–25. <https://doi.org/10.1056/NEJMoa2403211>.
[Article](https://doi.org/10.1056%2FNEJMoa2403211) [CAS](https://link.springer.com/articles/cas-redirect/1:CAS:528:DC%2BB2cXhvVCqs7fN) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=39018527) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC11687648) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Postacute%20sequelae%20of%20SARS-CoV-2%20infection%20in%20the%20Pre-Delta%2C%20Delta%2C%20and%20Omicron%20eras&journal=N%20Engl%20J%20Med&doi=10.1056%2FNEJMoa2403211&volume=391&pages=515-525&publication_year=2024&author=Xie%2CY&author=Choi%2CT&author=Al-Aly%2CZ)
9. Sherif ZA, Gomez CR, Connors TJ, Henrich TJ, Reeves WB, RECOVER Mechanistic Pathway Task Force. Pathogenic mechanisms of post-acute sequelae of SARS-CoV-2 infection (PASC). Elife. 2023;12:e86002. <https://doi.org/10.7554/eLife.86002>.
[Article](https://doi.org/10.7554%2FeLife.86002) [CAS](https://link.springer.com/articles/cas-redirect/1:CAS:528:DC%2BB2cXmtFans7c%3D) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=36947108) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC10032659) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Pathogenic%20mechanisms%20of%20post-acute%20sequelae%20of%20SARS-CoV-2%20infection%20%28PASC%29&journal=Elife&doi=10.7554%2FeLife.86002&volume=12&publication_year=2023&author=Sherif%2CZA&author=Gomez%2CCR&author=Connors%2CTJ&author=Henrich%2CTJ&author=Reeves%2CWB)
10. Mandel H, Yoo YJ, Allen AJ, Abedian S, Verzani Z, Karlson EW, et al. Long COVID incidence proportion in adults and children between 2020 and 2024: an EHR-based study from the RECOVER initiative. Clin Infect Dis. 2025. <https://doi.org/10.1093/cid/ciaf046>.
[Article](https://doi.org/10.1093%2Fcid%2Fciaf046) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=39907495) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC12272849) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Long%20COVID%20incidence%20proportion%20in%20adults%20and%20children%20between%202020%20and%202024%3A%20an%20EHR-based%20study%20from%20the%20RECOVER%20initiative&journal=Clin%20Infect%20Dis&doi=10.1093%2Fcid%2Fciaf046&publication_year=2025&author=Mandel%2CH&author=Yoo%2CYJ&author=Allen%2CAJ&author=Abedian%2CS&author=Verzani%2CZ&author=Karlson%2CEW)
11. Cai M, Xie Y, Topol EJ, Al-Aly Z. Three-year outcomes of post-acute sequelae of COVID-19. Nat Med. 2024;30:1564–73. <https://doi.org/10.1038/s41591-024-02987-8>.
[Article](https://doi.org/10.1038%2Fs41591-024-02987-8) [CAS](https://link.springer.com/articles/cas-redirect/1:CAS:528:DC%2BB2cXht1yhsLvJ) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=38816608) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC11186764) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Three-year%20outcomes%20of%20post-acute%20sequelae%20of%20COVID-19&journal=Nat%20Med&doi=10.1038%2Fs41591-024-02987-8&volume=30&pages=1564-1573&publication_year=2024&author=Cai%2CM&author=Xie%2CY&author=Topol%2CEJ&author=Al-Aly%2CZ)
12. Groff D, Sun A, Ssentongo AE, Ba DM, Parsons N, Poudel GR, et al. Short-term and long-term rates of postacute sequelae of SARS-CoV-2 infection: a systematic review. JAMA Netw Open. 2021;4:e2128568. <https://doi.org/10.1001/jamanetworkopen.2021.28568>.
[Article](https://doi.org/10.1001%2Fjamanetworkopen.2021.28568) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=34643720) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC8515212) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Short-term%20and%20long-term%20rates%20of%20postacute%20sequelae%20of%20SARS-CoV-2%20infection%3A%20a%20systematic%20review&journal=JAMA%20Netw%20Open&doi=10.1001%2Fjamanetworkopen.2021.28568&volume=4&publication_year=2021&author=Groff%2CD&author=Sun%2CA&author=Ssentongo%2CAE&author=Ba%2CDM&author=Parsons%2CN&author=Poudel%2CGR)
13. Kahlert CR, Strahm C, Güsewell S, Cusini A, Brucher A, Goppel S, et al. Post-acute sequelae after Severe Acute Respiratory Syndrome Coronavirus 2 infection by viral variant and vaccination status: a multicenter cross-sectional study. Clin Infect Dis. 2023;77:194–202. <https://doi.org/10.1093/cid/ciad143>.
[Article](https://doi.org/10.1093%2Fcid%2Fciad143) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=36905145) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC10371307) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Post-acute%20sequelae%20after%20Severe%20Acute%20Respiratory%20Syndrome%20Coronavirus%202%20infection%20by%20viral%20variant%20and%20vaccination%20status%3A%20a%20multicenter%20cross-sectional%20study&journal=Clin%20Infect%20Dis&doi=10.1093%2Fcid%2Fciad143&volume=77&pages=194-202&publication_year=2023&author=Kahlert%2CCR&author=Strahm%2CC&author=G%C3%BCsewell%2CS&author=Cusini%2CA&author=Brucher%2CA&author=Goppel%2CS)
14. Dörr T, Strahm C, Güsewell S, Ballouz T, Kocan E, Cusini A, et al. Burden of post–acute COVID-19 sequelae in healthcare workers and its course over a 30-month period–results from a prospective multicentre cohort. Infection. 2024. <https://doi.org/10.1007/s15010-024-02418-3>.
[Article](https://link.springer.com/doi/10.1007/s15010-024-02418-3) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=39532773) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC12316709) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Burden%20of%20post%E2%80%93acute%20COVID-19%20sequelae%20in%20healthcare%20workers%20and%20its%20course%20over%20a%2030-month%20period%E2%80%93results%20from%20a%20prospective%20multicentre%20cohort&journal=Infection&doi=10.1007%2Fs15010-024-02418-3&publication_year=2024&author=D%C3%B6rr%2CT&author=Strahm%2CC&author=G%C3%BCsewell%2CS&author=Ballouz%2CT&author=Kocan%2CE&author=Cusini%2CA)
15. Ballouz T, Menges D, Anagnostopoulos A, Domenghino A, Aschmann HE, Frei A, et al. Recovery and symptom trajectories up to two years after SARS-CoV-2 infection: population based, longitudinal cohort study. BMJ. 2023;381:e074425. <https://doi.org/10.1136/bmj-2022-074425>. (**British Medical Journal Publishing Group;**).
[Article](https://doi.org/10.1136%2Fbmj-2022-074425) [CAS](https://link.springer.com/articles/cas-redirect/1:CAS:528:DC%2BB2MXlt12ktbk%3D) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=37257891) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC10230608) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Recovery%20and%20symptom%20trajectories%20up%20to%20two%20years%20after%20SARS-CoV-2%20infection%3A%20population%20based%2C%20longitudinal%20cohort%20study&journal=BMJ&doi=10.1136%2Fbmj-2022-074425&volume=381&publication_year=2023&author=Ballouz%2CT&author=Menges%2CD&author=Anagnostopoulos%2CA&author=Domenghino%2CA&author=Aschmann%2CHE&author=Frei%2CA)
16. Foulkes S, Evans J, Neill C, Bishop J, Khawam J, Islam J, et al. Prevalence and impact of persistent symptoms following SARS-CoV-2 infection among healthcare workers: a cross-sectional survey in the SIREN cohort. J Infect. 2024;89:106259. <https://doi.org/10.1016/j.jinf.2024.106259>.
[Article](https://doi.org/10.1016%2Fj.jinf.2024.106259) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=39214242) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Prevalence%20and%20impact%20of%20persistent%20symptoms%20following%20SARS-CoV-2%20infection%20among%20healthcare%20workers%3A%20a%20cross-sectional%20survey%20in%20the%20SIREN%20cohort&journal=J%20Infect&doi=10.1016%2Fj.jinf.2024.106259&volume=89&publication_year=2024&author=Foulkes%2CS&author=Evans%2CJ&author=Neill%2CC&author=Bishop%2CJ&author=Khawam%2CJ&author=Islam%2CJ)
17. Lim SH, Lim YC, Zaki RA, Johari BM, Chang CY, Omar SFS, et al. Prevalence and predictors of post-acute COVID syndrome among infected healthcare workers at University Malaya Medical Centre. PLoS ONE. 2024;19:e0298376. <https://doi.org/10.1371/journal.pone.0298376>.
[Article](https://doi.org/10.1371%2Fjournal.pone.0298376) [CAS](https://link.springer.com/articles/cas-redirect/1:CAS:528:DC%2BB2cXpsVOqsr0%3D) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=38626017) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC11020391) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Prevalence%20and%20predictors%20of%20post-acute%20COVID%20syndrome%20among%20infected%20healthcare%20workers%20at%20University%20Malaya%20Medical%20Centre&journal=PLoS%20ONE&doi=10.1371%2Fjournal.pone.0298376&volume=19&publication_year=2024&author=Lim%2CSH&author=Lim%2CYC&author=Zaki%2CRA&author=Johari%2CBM&author=Chang%2CCY&author=Omar%2CSFS)
18. Dempsey B, Blake HA, Madan I, Stevelink SAM, Greenberg N, Raine R, et al. Post COVID-19 syndrome among 5248 healthcare workers in England: longitudinal findings from NHS CHECK. Occup Environ Med. 2024;81:471–9. <https://doi.org/10.1136/oemed-2024-109621>.
[Article](https://doi.org/10.1136%2Foemed-2024-109621) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=39358009) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC11503206) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Post%20COVID-19%20syndrome%20among%205248%20healthcare%20workers%20in%20England%3A%20longitudinal%20findings%20from%20NHS%20CHECK&journal=Occup%20Environ%20Med&doi=10.1136%2Foemed-2024-109621&volume=81&pages=471-479&publication_year=2024&author=Dempsey%2CB&author=Blake%2CHA&author=Madan%2CI&author=Stevelink%2CSAM&author=Greenberg%2CN&author=Raine%2CR)
19. Bowe B, Xie Y, Al-Aly Z. Postacute sequelae of COVID-19 at 2 years. Nat Med. 2023;29:2347–57. <https://doi.org/10.1038/s41591-023-02521-2>.
[Article](https://doi.org/10.1038%2Fs41591-023-02521-2) [CAS](https://link.springer.com/articles/cas-redirect/1:CAS:528:DC%2BB3sXhslektrrL) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=37605079) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC10504070) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Postacute%20sequelae%20of%20COVID-19%20at%202%20years&journal=Nat%20Med&doi=10.1038%2Fs41591-023-02521-2&volume=29&pages=2347-2357&publication_year=2023&author=Bowe%2CB&author=Xie%2CY&author=Al-Aly%2CZ)
20. Hurme A, Viinanen A, Teräsjärvi J, Jalkanen P, Feuth T, Löyttyniemi E, et al. Post-COVID-19 condition in prospective inpatient and outpatient cohorts. Sci Rep. 2025;15:6925. <https://doi.org/10.1038/s41598-025-90819-1>.
[Article](https://doi.org/10.1038%2Fs41598-025-90819-1) [CAS](https://link.springer.com/articles/cas-redirect/1:CAS:528:DC%2BB2MXlt1Wkt74%3D) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=40011519) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC11865615) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Post-COVID-19%20condition%20in%20prospective%20inpatient%20and%20outpatient%20cohorts&journal=Sci%20Rep&doi=10.1038%2Fs41598-025-90819-1&volume=15&publication_year=2025&author=Hurme%2CA&author=Viinanen%2CA&author=Ter%C3%A4sj%C3%A4rvi%2CJ&author=Jalkanen%2CP&author=Feuth%2CT&author=L%C3%B6yttyniemi%2CE)
21. Pfrommer LR, Diexer S, Klee B, Massag J, Gottschick C, Purschke O, et al. Post-COVID recovery is faster after an infection with the SARS-CoV-2 Omicron variant: a population-based cohort study. Infection. 2025;53:657–65. <https://doi.org/10.1007/s15010-024-02438-z>.
[Article](https://link.springer.com/doi/10.1007/s15010-024-02438-z) [CAS](https://link.springer.com/articles/cas-redirect/1:CAS:528:DC%2BB2cXisF2ntL3O) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=39556163) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Post-COVID%20recovery%20is%20faster%20after%20an%20infection%20with%20the%20SARS-CoV-2%20Omicron%20variant%3A%20a%20population-based%20cohort%20study&journal=Infection&doi=10.1007%2Fs15010-024-02438-z&volume=53&pages=657-665&publication_year=2025&author=Pfrommer%2CLR&author=Diexer%2CS&author=Klee%2CB&author=Massag%2CJ&author=Gottschick%2CC&author=Purschke%2CO)
22. Rahmati M, Udeh R, Kang J, Dolja‐Gore X, McEvoy M, Kazemi A, et al. Long‐term sequelae of COVID‐19: a systematic review and meta‐analysis of symptoms 3 years post‐SARS‐CoV‐2 infection. J Med Virol. 2025;97:e70429. <https://doi.org/10.1002/jmv.70429>.
[Article](https://doi.org/10.1002%2Fjmv.70429) [CAS](https://link.springer.com/articles/cas-redirect/1:CAS:528:DC%2BB2MXhtlKgsrfM) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=40476637) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC12143191) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Long%E2%80%90term%20sequelae%20of%20COVID%E2%80%9019%3A%20a%20systematic%20review%20and%20meta%E2%80%90analysis%20of%20symptoms%203%20years%20post%E2%80%90SARS%E2%80%90CoV%E2%80%902%20infection&journal=J%20Med%20Virol&doi=10.1002%2Fjmv.70429&volume=97&publication_year=2025&author=Rahmati%2CM&author=Udeh%2CR&author=Kang%2CJ&author=Dolja%E2%80%90Gore%2CX&author=McEvoy%2CM&author=Kazemi%2CA)
23. Vallée G, Xi D, Avramovic G, O’Kelly B, Lambert JS. Evaluating the longitudinal physical and psychological health effects of persistent long Covid 3.5 years after infection. PLoS ONE. 2025;20:e0326790. <https://doi.org/10.1371/journal.pone.0326790>.
[Article](https://doi.org/10.1371%2Fjournal.pone.0326790) [CAS](https://link.springer.com/articles/cas-redirect/1:CAS:528:DC%2BB2MXhsFemtb7P) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=40554575) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC12186912) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Evaluating%20the%20longitudinal%20physical%20and%20psychological%20health%20effects%20of%20persistent%20long%20Covid%203.5%20years%20after%20infection&journal=PLoS%20ONE&doi=10.1371%2Fjournal.pone.0326790&volume=20&publication_year=2025&author=Vall%C3%A9e%2CG&author=Xi%2CD&author=Avramovic%2CG&author=O%E2%80%99Kelly%2CB&author=Lambert%2CJS)
24. Gottlieb M, Yu H, Chen J, Spatz ES, Gentile NL, Geyer RE, et al. Differences in Long COVID severity by duration of illness, symptom evolution, and vaccination: a longitudinal cohort study from the INSPIRE group. Lancet Reg Health Am. 2025;44:101026. <https://doi.org/10.1016/j.lana.2025.101026>.
[Article](https://doi.org/10.1016%2Fj.lana.2025.101026) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=40040820) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC11875141) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Differences%20in%20Long%20COVID%20severity%20by%20duration%20of%20illness%2C%20symptom%20evolution%2C%20and%20vaccination%3A%20a%20longitudinal%20cohort%20study%20from%20the%20INSPIRE%20group&journal=Lancet%20Reg%20Health%20Am&doi=10.1016%2Fj.lana.2025.101026&volume=44&publication_year=2025&author=Gottlieb%2CM&author=Yu%2CH&author=Chen%2CJ&author=Spatz%2CES&author=Gentile%2CNL&author=Geyer%2CRE)
25. Ballouz T, Kerksieck P, Haile SR, Dressel H, Hämmig O, Bauer GF, et al. Work ability trajectories and sick leave in individuals with post COVID-19 condition: 3-year follow-up of a population-based cohort. Lancet Reg Health Eur. 2026;61:101536. <https://doi.org/10.1016/j.lanepe.2025.101536>.
[Article](https://doi.org/10.1016%2Fj.lanepe.2025.101536) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=41362299) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Work%20ability%20trajectories%20and%20sick%20leave%20in%20individuals%20with%20post%20COVID-19%20condition%3A%203-year%20follow-up%20of%20a%20population-based%20cohort&journal=Lancet%20Reg%20Health%20Eur&doi=10.1016%2Fj.lanepe.2025.101536&volume=61&publication_year=2026&author=Ballouz%2CT&author=Kerksieck%2CP&author=Haile%2CSR&author=Dressel%2CH&author=H%C3%A4mmig%2CO&author=Bauer%2CGF)
26. Kahlert CR, Persi R, Güsewell S, Egger T, Leal-Neto OB, Sumer J, et al. Non-occupational and occupational factors associated with specific SARS-CoV-2 antibodies among hospital workers – a multicentre cross-sectional study. Clin Microbiol Infect. 2021;27:1336–44. <https://doi.org/10.1016/j.cmi.2021.05.014>.
[Article](https://doi.org/10.1016%2Fj.cmi.2021.05.014) [CAS](https://link.springer.com/articles/cas-redirect/1:CAS:528:DC%2BB3MXhtlegsbjF) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=34020033) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC8131187) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Non-occupational%20and%20occupational%20factors%20associated%20with%20specific%20SARS-CoV-2%20antibodies%20among%20hospital%20workers%20%E2%80%93%20a%20multicentre%20cross-sectional%20study&journal=Clin%20Microbiol%20Infect&doi=10.1016%2Fj.cmi.2021.05.014&volume=27&pages=1336-1344&publication_year=2021&author=Kahlert%2CCR&author=Persi%2CR&author=G%C3%BCsewell%2CS&author=Egger%2CT&author=Leal-Neto%2COB&author=Sumer%2CJ)
27. Federal Office of Public Health. Virus variants overview. \[Internet\]. \[cited 2025 Apr 21\]. <https://www.covid19.admin.ch/en/epidemiologic/virus-variants>. Accessed 21 Apr 2025.
28. Coronavirus: Key Decisions of the Federal Council \[Internet\]. \[cited 2025 May 2\]. <https://www.uvek.admin.ch/uvek/de/home/uvek/coronavirus/wichtige-entscheide.html>. Accessed 2 May 2025.
29. Kohler P, Güsewell S, Seneghini M, Egger T, Leal O, Brucher A, et al. Impact of baseline SARS-CoV-2 antibody status on syndromic surveillance and the risk of subsequent COVID-19—a prospective multicenter cohort study. BMC Med. 2021;19:270. <https://doi.org/10.1186/s12916-021-02144-9>.
[Article](https://link.springer.com/doi/10.1186/s12916-021-02144-9) [CAS](https://link.springer.com/articles/cas-redirect/1:CAS:528:DC%2BB3MXit1OiurzF) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=34649585) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC8514323) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Impact%20of%20baseline%20SARS-CoV-2%20antibody%20status%20on%20syndromic%20surveillance%20and%20the%20risk%20of%20subsequent%20COVID-19%E2%80%94a%20prospective%20multicenter%20cohort%20study&journal=BMC%20Med&doi=10.1186%2Fs12916-021-02144-9&volume=19&publication_year=2021&author=Kohler%2CP&author=G%C3%BCsewell%2CS&author=Seneghini%2CM&author=Egger%2CT&author=Leal%2CO&author=Brucher%2CA)
30. Klok FA, Boon GJAM, Barco S, Endres M, Geelhoed JJM, Knauss S, et al. The Post-COVID-19 Functional Status scale: a tool to measure functional status over time after COVID-19. Eur Respir J. 2020;56:2001494. <https://doi.org/10.1183/13993003.01494-2020>.
[Article](https://doi.org/10.1183%2F13993003.01494-2020) [CAS](https://link.springer.com/articles/cas-redirect/1:CAS:528:DC%2BB3cXitVCjtLfN) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=32398306) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC7236834) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=The%20Post-COVID-19%20Functional%20Status%20scale%3A%20a%20tool%20to%20measure%20functional%20status%20over%20time%20after%20COVID-19&journal=Eur%20Respir%20J&doi=10.1183%2F13993003.01494-2020&volume=56&publication_year=2020&author=Klok%2CFA&author=Boon%2CGJAM&author=Barco%2CS&author=Endres%2CM&author=Geelhoed%2CJJM&author=Knauss%2CS)
31. Fernandez-de-las-Peñas C, Notarte KI, Macasaet R, Velasco JV, Catahay JA, Ver AT, et al. Persistence of post-COVID symptoms in the general population two years after SARS-CoV-2 infection: a systematic review and meta-analysis. J Infect. 2024;88:77–88. <https://doi.org/10.1016/j.jinf.2023.12.004>.
[Article](https://doi.org/10.1016%2Fj.jinf.2023.12.004) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=38101521) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Persistence%20of%20post-COVID%20symptoms%20in%20the%20general%20population%20two%20years%20after%20SARS-CoV-2%20infection%3A%20a%20systematic%20review%20and%20meta-analysis&journal=J%20Infect&doi=10.1016%2Fj.jinf.2023.12.004&volume=88&pages=77-88&publication_year=2024&author=Fernandez-de-las-Pe%C3%B1as%2CC&author=Notarte%2CKI&author=Macasaet%2CR&author=Velasco%2CJV&author=Catahay%2CJA&author=Ver%2CAT)
32. Kim Y, Bae S, Chang H-H, Kim S-W. Long COVID prevalence and impact on quality of life 2 years after acute COVID-19. Sci Rep. 2023;13:11207. <https://doi.org/10.1038/s41598-023-36995-4>.
[Article](https://doi.org/10.1038%2Fs41598-023-36995-4) [CAS](https://link.springer.com/articles/cas-redirect/1:CAS:528:DC%2BB3sXhsVKksrzM) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=37433819) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC10336045) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Long%20COVID%20prevalence%20and%20impact%20on%20quality%20of%20life%202%20years%20after%20acute%20COVID-19&journal=Sci%20Rep&doi=10.1038%2Fs41598-023-36995-4&volume=13&publication_year=2023&author=Kim%2CY&author=Bae%2CS&author=Chang%2CH-H&author=Kim%2CS-W)
33. Nguyen NN, Tissot-Dupont H, Brouqui P, Gautret P. Post-COVID syndrome in symptomatic COVID-19 patients: a retrospective cohort study. BMC Infect Dis. 2025;25:1099. <https://doi.org/10.1186/s12879-025-11360-0>.
[Article](https://link.springer.com/doi/10.1186/s12879-025-11360-0) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=40903751) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC12406458) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Post-COVID%20syndrome%20in%20symptomatic%20COVID-19%20patients%3A%20a%20retrospective%20cohort%20study&journal=BMC%20Infect%20Dis&doi=10.1186%2Fs12879-025-11360-0&volume=25&publication_year=2025&author=Nguyen%2CNN&author=Tissot-Dupont%2CH&author=Brouqui%2CP&author=Gautret%2CP)
34. Danesh V, Arroliga AC, Bourgeois JA, Boehm LM, McNeal MJ, Widmer AJ, et al. Symptom clusters seen in adult COVID-19 recovery clinic care seekers. J Gen Intern Med. 2023;38:442–9. <https://doi.org/10.1007/s11606-022-07908-4>.
[Article](https://link.springer.com/doi/10.1007/s11606-022-07908-4) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=36376627) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Symptom%20clusters%20seen%20in%20adult%20COVID-19%20recovery%20clinic%20care%20seekers&journal=J%20Gen%20Intern%20Med&doi=10.1007%2Fs11606-022-07908-4&volume=38&pages=442-449&publication_year=2023&author=Danesh%2CV&author=Arroliga%2CAC&author=Bourgeois%2CJA&author=Boehm%2CLM&author=McNeal%2CMJ&author=Widmer%2CAJ)
35. Huiberts AJ, De Bruijn S, Andeweg SP, Hoeve CE, Schipper M, De Melker HE, et al. Prospective cohort study of fatigue before and after SARS-CoV-2 infection in the Netherlands. Nat Commun. 2025;16:1923. <https://doi.org/10.1038/s41467-025-56994-5>.
[Article](https://doi.org/10.1038%2Fs41467-025-56994-5) [CAS](https://link.springer.com/articles/cas-redirect/1:CAS:528:DC%2BB2MXlslSkurs%3D) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=40038286) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC11880519) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Prospective%20cohort%20study%20of%20fatigue%20before%20and%20after%20SARS-CoV-2%20infection%20in%20the%20Netherlands&journal=Nat%20Commun&doi=10.1038%2Fs41467-025-56994-5&volume=16&publication_year=2025&author=Huiberts%2CAJ&author=Bruijn%2CS&author=Andeweg%2CSP&author=Hoeve%2CCE&author=Schipper%2CM&author=Melker%2CHE)
36. Strahm C, Seneghini M, Güsewell S, Egger T, Leal-Neto O, Brucher A, et al. Symptoms compatible with long coronavirus disease (COVID) in healthcare workers with and without severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection—results of a prospective multicenter cohort. Clin Infect Dis. 2022;75:e1011–9. <https://doi.org/10.1093/cid/ciac054>.
[Article](https://doi.org/10.1093%2Fcid%2Fciac054) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=35090015) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC9383387) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Symptoms%20compatible%20with%20long%20coronavirus%20disease%20%28COVID%29%20in%20healthcare%20workers%20with%20and%20without%20severe%20acute%20respiratory%20syndrome%20coronavirus%202%20%28SARS-CoV-2%29%20infection%E2%80%94results%20of%20a%20prospective%20multicenter%20cohort&journal=Clin%20Infect%20Dis&doi=10.1093%2Fcid%2Fciac054&volume=75&pages=e1011-e1019&publication_year=2022&author=Strahm%2CC&author=Seneghini%2CM&author=G%C3%BCsewell%2CS&author=Egger%2CT&author=Leal-Neto%2CO&author=Brucher%2CA)
37. Nakagama Y, Komase Y, Kaku N, Nitahara Y, Tshibangu-Kabamba E, Tominaga T, et al. Detecting waning serological response with commercial immunoassays: 18-month longitudinal follow-up of anti-SARS-CoV-2 Nucleocapsid antibodies. Microbiol Spectr. 2022;10:e00986-22. <https://doi.org/10.1128/spectrum.00986-22>.
[Article](https://doi.org/10.1128%2Fspectrum.00986-22) [CAS](https://link.springer.com/articles/cas-redirect/1:CAS:528:DC%2BB38XisVyqt73M) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=35867423) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC9430644) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Detecting%20waning%20serological%20response%20with%20commercial%20immunoassays%3A%2018-month%20longitudinal%20follow-up%20of%20anti-SARS-CoV-2%20Nucleocapsid%20antibodies&journal=Microbiol%20Spectr&doi=10.1128%2Fspectrum.00986-22&volume=10&publication_year=2022&author=Nakagama%2CY&author=Komase%2CY&author=Kaku%2CN&author=Nitahara%2CY&author=Tshibangu-Kabamba%2CE&author=Tominaga%2CT)
[Download references](https://citation-needed.springer.com/v2/references/10.1007/s15010-026-02768-0?format=refman&flavour=references)
## Acknowledgements
The SURPRISE+ Study Group: Alexia Cusini, Cantonal Hospital Graubuenden, Chur, Switzerland; Tamara Dörr, HOCH, Cantonal Hospital St.Gallen, Division of Infectious Diseases, Infection Prevention and Travel Medicine, St.Gallen, Switzerland; Stephan Goppel, Psychiatry Services of the Canton of St Gallen, St Gallen, Switzerland; Fabian Grässli, HOCH, Cantonal Hospital St.Gallen, Division of Infectious Diseases, Infection Prevention and Travel Medicine, St.Gallen, Switzerland, Christian R. Kahlert; HOCH, Cantonal Hospital St.Gallen, Division of Infectious Diseases, Infection Prevention and Travel Medicine, St.Gallen, Switzerland and Department of InfectiousDiseases and Hospital Epidemiology, Children’s Hospital of EasternSwitzerland,St. Gallen, Switzerland; Joelle Keller, Hirslanden Clinic Zurich, Zurich, Switzerland; Simone Kessler, HOCH, Cantonal Hospital St.Gallen, Division of Infectious Diseases, Infection Prevention and Travel Medicine, St.Gallen, Switzerland; Philipp Kohler, HOCH, Cantonal Hospital St.Gallen, Division of Infectious Diseases, Infection Prevention and Travel Medicine, St.Gallen, Switzerland and Epidemiology, Biostatistics and Prevention Institute (EBPI), University of Zurich, Zurich, Switzerland; Stefan P. Kuster, HOCH, Cantonal Hospital St.Gallen, Division of Infectious Diseases, Infection Prevention and Travel Medicine, St.Gallen, Switzerland; J. Carsten Möller, Center for Neurological Rehabilitation Zihlschlacht, Zihlschlacht, Switzerland; Maja F. Müller, Hirslanden Clinic Zurich, Zurich, Switzerland; Philip Rieder, Hirslanden Clinic Zurich, Zurich, Switzerland; Lorenz Risch, Labormedizinisches Zentrum Dr Risch Ostschweiz AG, Buchs, Switzerland, Private Universität im Fürstentum Liechtenstein, Triesen, Liechtenstein and Center of Laboratory Medicine, Institute of Clinical Chemistry, University of Bern, Inselspital, Bern, Switzerland; Markus Rütti, HOCH, Hospital Wil, Division of Internal Medicine, St. Gallen, Switzerland; Matthias Schlegel, HOCH, Cantonal Hospital St.Gallen, Division of Infectious Diseases, Infection Prevention and Travel Medicine, St.Gallen, Switzerland; Reto Stocker, Hirslanden Clinic Zurich, Zurich, Switzerland and Foundation Quality of Life, Zurich, Switzerland; Matthias von Kietzell, Hirslanden Clinic Stephanshorn, St. Gallen, Switzerland; Danielle Vuichard-Gysin, Thurgau Hospital Group, Division of Infectious Diseases and Hospital Epidemiology, Muensterlingen and Frauenfeld, Switzerland; Department of Research and Development, Swiss National Centre for Infection Prevention (Swissnoso), Bern, Switzerland; Geriatric Clinic St. Gallen, St. Gallen, Switzerland.
## Funding
This work was supported by the Swiss National Sciences Foundation SNSF (grant number 31CA30\_196544; grant number PZ00P3\_179919 to PK).
## Author information
Author notes
1. Tamara Dörr and Philipp Kohler equal contribution as last authors.
### Authors and Affiliations
1. Division of Infectious Diseases, Infection Prevention and Travel Medicine, HOCH, Cantonal Hospital St.Gallen, Rorschacher Strasse 95, 9007, St. Gallen, Switzerland
Christian R. Kahlert, Stefan P. Kuster, Matthias Schlegel, Carol Strahm, Tamara Dörr & Philipp Kohler
2. Epidemiology, Biostatistics and Prevention Institute (EBPI), University of Zurich, Hirschengraben 84, 8001, Zurich, Switzerland
Philipp Saurer, Tala Ballouz, Sarah R. Haile, Milo A. Puhan & Philipp Kohler
3. Cantonal Hospital Graubuenden, Chur, Switzerland
Alexia Cusini
4. Hirslanden Clinic Stephanshorn, St. Gallen, Switzerland
Matthias von Kietzell
5. Division of Internal Medicine, HOCH, Hospital Wil, St. Gallen, Switzerland
Markus Rütti
6. Hirslanden Clinic Zurich, Zurich, Switzerland
Reto Stocker
7. Division of Infectious Diseases and Hospital Epidemiology, Thurgau Hospital Group, Muensterlingen, Frauenfeld, Switzerland
Danielle Vuichard-Gysin
8. Department of Research and Development, Swiss National Centre for Infection Prevention (Swissnoso), Bern, Switzerland
Danielle Vuichard-Gysin
9. Department of Infectious Diseases and Hospital Epidemiology, Children’s Hospital of Eastern Switzerland, St. Gallen, Switzerland
Christian R. Kahlert
10. Labormedizinisches Zentrum Dr Risch Ostschweiz AG, Buchs, Switzerland
Lorenz Risch
11. Private Universität im Fürstentum Liechtenstein, Triesen, Liechtenstein
Lorenz Risch
12. Center of Laboratory Medicine, Institute of Clinical Chemistry, University of Bern, Inselspital, Bern, Switzerland
Lorenz Risch
13. Foundation Quality of Life, Zurich, Switzerland
Reto Stocker
Authors
1. Philipp Saurer
[View author publications](https://link.springer.com/search?sortBy=newestFirst&contributor=Philipp%20Saurer)
Search author on:[PubMed](https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=search&term=Philipp%20Saurer) [Google Scholar](https://scholar.google.co.uk/scholar?as_q=&num=10&btnG=Search+Scholar&as_epq=&as_oq=&as_eq=&as_occt=any&as_sauthors=%22Philipp%20Saurer%22&as_publication=&as_ylo=&as_yhi=&as_allsubj=all&hl=en)
2. Tala Ballouz
[View author publications](https://link.springer.com/search?sortBy=newestFirst&contributor=Tala%20Ballouz)
Search author on:[PubMed](https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=search&term=Tala%20Ballouz) [Google Scholar](https://scholar.google.co.uk/scholar?as_q=&num=10&btnG=Search+Scholar&as_epq=&as_oq=&as_eq=&as_occt=any&as_sauthors=%22Tala%20Ballouz%22&as_publication=&as_ylo=&as_yhi=&as_allsubj=all&hl=en)
3. Alexia Cusini
[View author publications](https://link.springer.com/search?sortBy=newestFirst&contributor=Alexia%20Cusini)
Search author on:[PubMed](https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=search&term=Alexia%20Cusini) [Google Scholar](https://scholar.google.co.uk/scholar?as_q=&num=10&btnG=Search+Scholar&as_epq=&as_oq=&as_eq=&as_occt=any&as_sauthors=%22Alexia%20Cusini%22&as_publication=&as_ylo=&as_yhi=&as_allsubj=all&hl=en)
4. Sarah R. Haile
[View author publications](https://link.springer.com/search?sortBy=newestFirst&contributor=Sarah%20R.%20Haile)
Search author on:[PubMed](https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=search&term=Sarah%20R.%20Haile) [Google Scholar](https://scholar.google.co.uk/scholar?as_q=&num=10&btnG=Search+Scholar&as_epq=&as_oq=&as_eq=&as_occt=any&as_sauthors=%22Sarah%20R.%20Haile%22&as_publication=&as_ylo=&as_yhi=&as_allsubj=all&hl=en)
5. Christian R. Kahlert
[View author publications](https://link.springer.com/search?sortBy=newestFirst&contributor=Christian%20R.%20Kahlert)
Search author on:[PubMed](https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=search&term=Christian%20R.%20Kahlert) [Google Scholar](https://scholar.google.co.uk/scholar?as_q=&num=10&btnG=Search+Scholar&as_epq=&as_oq=&as_eq=&as_occt=any&as_sauthors=%22Christian%20R.%20Kahlert%22&as_publication=&as_ylo=&as_yhi=&as_allsubj=all&hl=en)
6. Matthias von Kietzell
[View author publications](https://link.springer.com/search?sortBy=newestFirst&contributor=Matthias%20von%20Kietzell)
Search author on:[PubMed](https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=search&term=Matthias%20von%20Kietzell) [Google Scholar](https://scholar.google.co.uk/scholar?as_q=&num=10&btnG=Search+Scholar&as_epq=&as_oq=&as_eq=&as_occt=any&as_sauthors=%22Matthias%20von%20Kietzell%22&as_publication=&as_ylo=&as_yhi=&as_allsubj=all&hl=en)
7. Stefan P. Kuster
[View author publications](https://link.springer.com/search?sortBy=newestFirst&contributor=Stefan%20P.%20Kuster)
Search author on:[PubMed](https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=search&term=Stefan%20P.%20Kuster) [Google Scholar](https://scholar.google.co.uk/scholar?as_q=&num=10&btnG=Search+Scholar&as_epq=&as_oq=&as_eq=&as_occt=any&as_sauthors=%22Stefan%20P.%20Kuster%22&as_publication=&as_ylo=&as_yhi=&as_allsubj=all&hl=en)
8. Markus Rütti
[View author publications](https://link.springer.com/search?sortBy=newestFirst&contributor=Markus%20R%C3%BCtti)
Search author on:[PubMed](https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=search&term=Markus%20R%C3%BCtti) [Google Scholar](https://scholar.google.co.uk/scholar?as_q=&num=10&btnG=Search+Scholar&as_epq=&as_oq=&as_eq=&as_occt=any&as_sauthors=%22Markus%20R%C3%BCtti%22&as_publication=&as_ylo=&as_yhi=&as_allsubj=all&hl=en)
9. Matthias Schlegel
[View author publications](https://link.springer.com/search?sortBy=newestFirst&contributor=Matthias%20Schlegel)
Search author on:[PubMed](https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=search&term=Matthias%20Schlegel) [Google Scholar](https://scholar.google.co.uk/scholar?as_q=&num=10&btnG=Search+Scholar&as_epq=&as_oq=&as_eq=&as_occt=any&as_sauthors=%22Matthias%20Schlegel%22&as_publication=&as_ylo=&as_yhi=&as_allsubj=all&hl=en)
10. Carol Strahm
[View author publications](https://link.springer.com/search?sortBy=newestFirst&contributor=Carol%20Strahm)
Search author on:[PubMed](https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=search&term=Carol%20Strahm) [Google Scholar](https://scholar.google.co.uk/scholar?as_q=&num=10&btnG=Search+Scholar&as_epq=&as_oq=&as_eq=&as_occt=any&as_sauthors=%22Carol%20Strahm%22&as_publication=&as_ylo=&as_yhi=&as_allsubj=all&hl=en)
11. Reto Stocker
[View author publications](https://link.springer.com/search?sortBy=newestFirst&contributor=Reto%20Stocker)
Search author on:[PubMed](https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=search&term=Reto%20Stocker) [Google Scholar](https://scholar.google.co.uk/scholar?as_q=&num=10&btnG=Search+Scholar&as_epq=&as_oq=&as_eq=&as_occt=any&as_sauthors=%22Reto%20Stocker%22&as_publication=&as_ylo=&as_yhi=&as_allsubj=all&hl=en)
12. Danielle Vuichard-Gysin
[View author publications](https://link.springer.com/search?sortBy=newestFirst&contributor=Danielle%20Vuichard-Gysin)
Search author on:[PubMed](https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=search&term=Danielle%20Vuichard-Gysin) [Google Scholar](https://scholar.google.co.uk/scholar?as_q=&num=10&btnG=Search+Scholar&as_epq=&as_oq=&as_eq=&as_occt=any&as_sauthors=%22Danielle%20Vuichard-Gysin%22&as_publication=&as_ylo=&as_yhi=&as_allsubj=all&hl=en)
13. Lorenz Risch
[View author publications](https://link.springer.com/search?sortBy=newestFirst&contributor=Lorenz%20Risch)
Search author on:[PubMed](https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=search&term=Lorenz%20Risch) [Google Scholar](https://scholar.google.co.uk/scholar?as_q=&num=10&btnG=Search+Scholar&as_epq=&as_oq=&as_eq=&as_occt=any&as_sauthors=%22Lorenz%20Risch%22&as_publication=&as_ylo=&as_yhi=&as_allsubj=all&hl=en)
14. Milo A. Puhan
[View author publications](https://link.springer.com/search?sortBy=newestFirst&contributor=Milo%20A.%20Puhan)
Search author on:[PubMed](https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=search&term=Milo%20A.%20Puhan) [Google Scholar](https://scholar.google.co.uk/scholar?as_q=&num=10&btnG=Search+Scholar&as_epq=&as_oq=&as_eq=&as_occt=any&as_sauthors=%22Milo%20A.%20Puhan%22&as_publication=&as_ylo=&as_yhi=&as_allsubj=all&hl=en)
15. Tamara Dörr
[View author publications](https://link.springer.com/search?sortBy=newestFirst&contributor=Tamara%20D%C3%B6rr)
Search author on:[PubMed](https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=search&term=Tamara%20D%C3%B6rr) [Google Scholar](https://scholar.google.co.uk/scholar?as_q=&num=10&btnG=Search+Scholar&as_epq=&as_oq=&as_eq=&as_occt=any&as_sauthors=%22Tamara%20D%C3%B6rr%22&as_publication=&as_ylo=&as_yhi=&as_allsubj=all&hl=en)
16. Philipp Kohler
[View author publications](https://link.springer.com/search?sortBy=newestFirst&contributor=Philipp%20Kohler)
Search author on:[PubMed](https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=search&term=Philipp%20Kohler) [Google Scholar](https://scholar.google.co.uk/scholar?as_q=&num=10&btnG=Search+Scholar&as_epq=&as_oq=&as_eq=&as_occt=any&as_sauthors=%22Philipp%20Kohler%22&as_publication=&as_ylo=&as_yhi=&as_allsubj=all&hl=en)
### Consortia
### on behalf of the SURPRISE+ cohort
- Alexia Cusini
- , Tamara Dörr
- , Stephan Goppel
- , Fabian Grässli
- , Christian R. Kahlert
- , Joelle Keller
- , Simone Kessler
- , Philipp Kohler
- , Stefan P. Kuster
- , J. Carsten Möller
- , Maja F. Müller
- , Philip Rieder
- , Lorenz Risch
- , Markus Rütti
- , Matthias Schlegel
- , Reto Stocker
- , Matthias von Kietzell
- & Danielle Vuichard-Gysin
### Contributions
All authors contributed to the study conception and design. Data collection was performed by the SURPRISE + Study Group. Data analyses were performed by P.S. The first draft of the manuscript was written by P.S. and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript. T.D. and P.K. contributed equally as last authors.
### Corresponding authors
Correspondence to [Philipp Saurer](mailto:philippdaniel.saurer@uzh.ch) or [Philipp Kohler](mailto:philipp.kohler@h-och.ch).
## Ethics declarations
### Conflict of interest
The authors declare no competing interests.
### Ethical approval
The study protocol was approved by the Ethics Committee of Eastern Switzerland (\#2020–00502).
### Consent to participate
All participants provided electronic informed consent.
## Supplementary Information
Below is the link to the electronic supplementary material.
### [Supplementary file1 (DOCX 1137 kb) (download DOCX )](https://static-content.springer.com/esm/art%3A10.1007%2Fs15010-026-02768-0/MediaObjects/15010_2026_2768_MOESM1_ESM.docx)
## Rights and permissions
**Open Access** This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit <http://creativecommons.org/licenses/by-nc-nd/4.0/>.
[Reprints and permissions](https://s100.copyright.com/AppDispatchServlet?title=Persistence%20of%20Post-Acute%20COVID-19%20Sequelae%20%28PASC%29%20symptoms%20in%20healthcare%20workers%20four%20years%20after%20ancestral%20SARS-CoV-2%20infection%3A%20a%20prospective%20multicentre%20cohort&author=Philipp%20Saurer%20Stephan%20Goppel%20et%20al&contentID=10.1007%2Fs15010-026-02768-0©right=The%20Author%28s%29&publication=0300-8126&publicationDate=2026-03-17&publisherName=SpringerNature&orderBeanReset=true&oa=CC%20BY-NC-ND)
## About this article
[](https://crossmark.crossref.org/dialog/?doi=10.1007/s15010-026-02768-0)
### Cite this article
Saurer, P., Ballouz, T., Cusini, A. *et al.* Persistence of Post-Acute COVID-19 Sequelae (PASC) symptoms in healthcare workers four years after ancestral SARS-CoV-2 infection: a prospective multicentre cohort. *Infection* (2026). https://doi.org/10.1007/s15010-026-02768-0
[Download citation](https://citation-needed.springer.com/v2/references/10.1007/s15010-026-02768-0?format=refman&flavour=citation)
- Received: 22 December 2025
- Accepted: 10 March 2026
- Published: 17 March 2026
- Version of record: 17 March 2026
- DOI: https://doi.org/10.1007/s15010-026-02768-0
### Share this article
Anyone you share the following link with will be able to read this content:
Get shareable link
Sorry, a shareable link is not currently available for this article.
Copy shareable link to clipboard
Provided by the Springer Nature SharedIt content-sharing initiative
### Keywords
- [Post-Acute COVID-19 Sequelae (PASC)](https://link.springer.com/search?query=Post-Acute%20COVID-19%20Sequelae%20%28PASC%29&facet-discipline="Medicine%20%26%20Public%20Health")
- [Long COVID](https://link.springer.com/search?query=Long%20COVID&facet-discipline="Medicine%20%26%20Public%20Health")
- [Symptom prevalence](https://link.springer.com/search?query=Symptom%20prevalence&facet-discipline="Medicine%20%26%20Public%20Health")
- [Healthcare workers](https://link.springer.com/search?query=Healthcare%20workers&facet-discipline="Medicine%20%26%20Public%20Health")
- [Ancestral SARS-CoV-2](https://link.springer.com/search?query=Ancestral%20SARS-CoV-2&facet-discipline="Medicine%20%26%20Public%20Health")
### Profiles
1. Philipp Saurer
[View author profile](https://link.springer.com/researchers/19810954SN)
2. Philipp Kohler
[View author profile](https://link.springer.com/researchers/71593230SN)
Advertisement
## Search
## Navigation
- [Find a journal](https://link.springer.com/journals/)
- [Publish with us](https://www.springernature.com/gp/authors)
- [Track your research](https://link.springernature.com/home/)
### Discover content
- [Journals A-Z](https://link.springer.com/journals/a/1)
- [Books A-Z](https://link.springer.com/books/a/1)
### Publish with us
- [Journal finder](https://link.springer.com/journals)
- [Publish your research](https://www.springernature.com/gp/authors)
- [Language editing](https://authorservices.springernature.com/go/sn/?utm_source=SNLinkfooter&utm_medium=Web&utm_campaign=SNReferral)
- [Open access publishing](https://www.springernature.com/gp/open-science/about/the-fundamentals-of-open-access-and-open-research)
### Products and services
- [Our products](https://www.springernature.com/gp/products)
- [Librarians](https://www.springernature.com/gp/librarians)
- [Societies](https://www.springernature.com/gp/societies)
- [Partners and advertisers](https://www.springernature.com/gp/partners)
### Our brands
- [Springer](https://link.springer.com/brands/springer)
- [Nature Portfolio](https://www.nature.com/)
- [BMC](https://link.springer.com/brands/bmc)
- [Palgrave Macmillan](https://link.springer.com/brands/palgrave)
- [Apress](https://link.springer.com/brands/apress)
- [Discover](https://link.springer.com/brands/discover)
- Your privacy choices/Manage cookies
- [Your US state privacy rights](https://www.springernature.com/gp/legal/ccpa)
- [Accessibility statement](https://link.springer.com/accessibility)
- [Terms and conditions](https://link.springer.com/termsandconditions)
- [Privacy policy](https://link.springer.com/privacystatement)
- [Help and support](https://support.springernature.com/en/support/home)
- [Legal notice](https://link.springer.com/legal-notice)
- [Cancel contracts here](https://support.springernature.com/en/support/solutions/articles/6000255911-subscription-cancellations)
Not affiliated
[](https://www.springernature.com/)
© 2026 Springer Nature |
| Readable Markdown | ## Abstract
### Purpose
Post-Acute Sequelae of SARS-CoV-2 Infection (PASC), or long COVID (LC), remains a significant burden for public health, with limited long-term data. This study aimed to assess the prevalence and evolution of PASC symptoms after ancestral SARS-CoV-2 (aSCV2) infection in a longitudinal healthcare worker (HCW) cohort.
### Methods
A multicentre cohort study involving HCWs from 14 institutions was conducted in Switzerland. Infection status was based on self-reported positive swabs, with additional serology used to confirm uninfected controls. Baseline was defined as the first survey conducted in 2022 (median 18.5 months post-infection), with follow-up surveys every 6 months through November 2024. To identify PASC-specific symptoms, 24 chronic symptoms were compared between 456 aSCV2-infected and 571 uninfected participants using chi-square tests at baseline. In aSCV2-infected individuals reporting PASC-specific symptoms, symptom trajectories and subjective LC were analyzed across follow-up surveys. Functional limitations were assessed using the Post-COVID Functional Status (PCFS) scale.
### Results
Thirteen of 24 symptoms were more common in aSCV2-infected individuals, with fatigue (22.8%), loss of smell/taste (11.4%), and brain fog (8.3%) being most prevalent. At baseline, 186/456 (40.8%) infected participants reported ≥ 1 PASC-specific symptom. Most symptoms declined in prevalence up to the last survey (median 47.5 months post-infection), although 41/70 (58.6%) remaining participants still reported ≥ 1 PASC symptom. Subjective LC was reported by 70/186 (37.6%) and was associated with higher symptom burden. PCFS scores showed slight impairments in most cases, although moderate-to-severe limitations often persisted.
### Conclusions
PASC symptoms persisted up to four years after aSCV2 infection in a substantial proportion of HCWs.
### Similar content being viewed by others



## Introduction
Although acute SARS-CoV-2 infection has caused significant mortality and morbidity, attention has increasingly shifted to its long-term effects, commonly referred to as Post-Acute Sequelae of SARS-CoV-2 Infection (PASC) or long COVID (LC). PASC is defined as symptoms that persist or newly develop at least three months after acute infection, last for at least two months, and cannot be explained by alternative diagnoses \[[1](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR1 "Post COVID-19 condition (Long COVID) [Internet].
https://www.who.int/europe/news-room/fact-sheets/item/post-covid-19-condition
. Accessed 15 Jan 2025."), [2](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR2 "Parums DV. Long COVID or Post-Acute Sequelae of SARS-CoV-2 Infection (PASC) and the urgent need to identify diagnostic biomarkers and risk factors. Med Sci Monit. 2024.
https://doi.org/10.12659/MSM.946512
.")\]. It includes a wide range of symptoms affecting multiple organ systems, with fatigue, cognitive dysfunction, and respiratory symptoms being most common \[[3](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR3 "Davis HE, McCorkell L, Vogel JM, Topol EJ. Long COVID: major findings, mechanisms and recommendations. Nat Rev Microbiol. 2023;21:133–46.
https://doi.org/10.1038/s41579-022-00846-2
."),[4](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR4 "Reese JT, Blau H, Casiraghi E, Bergquist T, Loomba JJ, Callahan TJ, et al. Generalisable long COVID subtypes: findings from the NIH N3C and RECOVER programmes. EBioMedicine. 2023;87:104413.
https://doi.org/10.1016/j.ebiom.2022.104413
."),[5](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR5 "Thaweethai T, Jolley SE, Karlson EW, Levitan EB, Levy B, McComsey GA, et al. Development of a definition of postacute sequelae of SARS-CoV-2 infection. JAMA. 2023;329:1934.
https://doi.org/10.1001/jama.2023.8823
."),[6](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR6 "Griffin DO. Postacute sequelae of COVID (PASC or Long COVID): an evidenced-based approach. Open Forum Infect Dis. 2024;11:ofae462.
https://doi.org/10.1093/ofid/ofae462
."),[7](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR7 "Hastie CE, Lowe DJ, McAuley A, Mills NL, Winter AJ, Black C, et al. True prevalence of long-COVID in a nationwide, population cohort study. Nat Commun. 2023;14:7892.
https://doi.org/10.1038/s41467-023-43661-w
."),[8](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR8 "Xie Y, Choi T, Al-Aly Z. Postacute sequelae of SARS-CoV-2 infection in the Pre-Delta, Delta, and Omicron eras. N Engl J Med. 2024;391:515–25.
https://doi.org/10.1056/NEJMoa2403211
."),[9](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR9 "Sherif ZA, Gomez CR, Connors TJ, Henrich TJ, Reeves WB, RECOVER Mechanistic Pathway Task Force. Pathogenic mechanisms of post-acute sequelae of SARS-CoV-2 infection (PASC). Elife. 2023;12:e86002.
https://doi.org/10.7554/eLife.86002
.")\]. However, many of these symptoms also occur in non-infected individuals and are not specific for PASC. Additionally, not all individuals reporting PASC symptoms consider themselves to suffer from LC, highlighting the heterogeneity of post-COVID outcomes and the challenges of their assessment. Prevalence estimates of PASC vary across studies, ranging from 3 to 54%, depending on the PASC definition, population, sampling scheme, severity and time since initial infection, vaccination status, as well as the viral variant \[[5](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR5 "Thaweethai T, Jolley SE, Karlson EW, Levitan EB, Levy B, McComsey GA, et al. Development of a definition of postacute sequelae of SARS-CoV-2 infection. JAMA. 2023;329:1934.
https://doi.org/10.1001/jama.2023.8823
."), [8](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR8 "Xie Y, Choi T, Al-Aly Z. Postacute sequelae of SARS-CoV-2 infection in the Pre-Delta, Delta, and Omicron eras. N Engl J Med. 2024;391:515–25.
https://doi.org/10.1056/NEJMoa2403211
."), [10](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR10 "Mandel H, Yoo YJ, Allen AJ, Abedian S, Verzani Z, Karlson EW, et al. Long COVID incidence proportion in adults and children between 2020 and 2024: an EHR-based study from the RECOVER initiative. Clin Infect Dis. 2025.
https://doi.org/10.1093/cid/ciaf046
."),[11](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR11 "Cai M, Xie Y, Topol EJ, Al-Aly Z. Three-year outcomes of post-acute sequelae of COVID-19. Nat Med. 2024;30:1564–73.
https://doi.org/10.1038/s41591-024-02987-8
."),[12](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR12 "Groff D, Sun A, Ssentongo AE, Ba DM, Parsons N, Poudel GR, et al. Short-term and long-term rates of postacute sequelae of SARS-CoV-2 infection: a systematic review. JAMA Netw Open. 2021;4:e2128568.
https://doi.org/10.1001/jamanetworkopen.2021.28568
."),[13](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR13 "Kahlert CR, Strahm C, Güsewell S, Cusini A, Brucher A, Goppel S, et al. Post-acute sequelae after Severe Acute Respiratory Syndrome Coronavirus 2 infection by viral variant and vaccination status: a multicenter cross-sectional study. Clin Infect Dis. 2023;77:194–202.
https://doi.org/10.1093/cid/ciad143
."),[14](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR14 "Dörr T, Strahm C, Güsewell S, Ballouz T, Kocan E, Cusini A, et al. Burden of post–acute COVID-19 sequelae in healthcare workers and its course over a 30-month period–results from a prospective multicentre cohort. Infection. 2024.
https://doi.org/10.1007/s15010-024-02418-3
."),[15](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR15 "Ballouz T, Menges D, Anagnostopoulos A, Domenghino A, Aschmann HE, Frei A, et al. Recovery and symptom trajectories up to two years after SARS-CoV-2 infection: population based, longitudinal cohort study. BMJ. 2023;381:e074425.
https://doi.org/10.1136/bmj-2022-074425
. (British Medical Journal Publishing Group;).")\]. Comparative analyses show that the risk of developing PASC is highest after infection with ancestral SARS-CoV-2 (aSCV2) and decreases with subsequent variants \[[5](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR5 "Thaweethai T, Jolley SE, Karlson EW, Levitan EB, Levy B, McComsey GA, et al. Development of a definition of postacute sequelae of SARS-CoV-2 infection. JAMA. 2023;329:1934.
https://doi.org/10.1001/jama.2023.8823
."), [8](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR8 "Xie Y, Choi T, Al-Aly Z. Postacute sequelae of SARS-CoV-2 infection in the Pre-Delta, Delta, and Omicron eras. N Engl J Med. 2024;391:515–25.
https://doi.org/10.1056/NEJMoa2403211
."), [13](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR13 "Kahlert CR, Strahm C, Güsewell S, Cusini A, Brucher A, Goppel S, et al. Post-acute sequelae after Severe Acute Respiratory Syndrome Coronavirus 2 infection by viral variant and vaccination status: a multicenter cross-sectional study. Clin Infect Dis. 2023;77:194–202.
https://doi.org/10.1093/cid/ciad143
.")\].
During the aSCV2-dominant period of the pandemic, health care workers (HCWs) were particularly affected by PASC due to their increased exposure to SARS-CoV-2, with prevalence rates noticeably higher than those observed in the general population \[[13](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR13 "Kahlert CR, Strahm C, Güsewell S, Cusini A, Brucher A, Goppel S, et al. Post-acute sequelae after Severe Acute Respiratory Syndrome Coronavirus 2 infection by viral variant and vaccination status: a multicenter cross-sectional study. Clin Infect Dis. 2023;77:194–202.
https://doi.org/10.1093/cid/ciad143
."), [14](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR14 "Dörr T, Strahm C, Güsewell S, Ballouz T, Kocan E, Cusini A, et al. Burden of post–acute COVID-19 sequelae in healthcare workers and its course over a 30-month period–results from a prospective multicentre cohort. Infection. 2024.
https://doi.org/10.1007/s15010-024-02418-3
."), [16](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR16 "Foulkes S, Evans J, Neill C, Bishop J, Khawam J, Islam J, et al. Prevalence and impact of persistent symptoms following SARS-CoV-2 infection among healthcare workers: a cross-sectional survey in the SIREN cohort. J Infect. 2024;89:106259.
https://doi.org/10.1016/j.jinf.2024.106259
."),[17](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR17 "Lim SH, Lim YC, Zaki RA, Johari BM, Chang CY, Omar SFS, et al. Prevalence and predictors of post-acute COVID syndrome among infected healthcare workers at University Malaya Medical Centre. PLoS ONE. 2024;19:e0298376.
https://doi.org/10.1371/journal.pone.0298376
."),[18](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR18 "Dempsey B, Blake HA, Madan I, Stevelink SAM, Greenberg N, Raine R, et al. Post COVID-19 syndrome among 5248 healthcare workers in England: longitudinal findings from NHS CHECK. Occup Environ Med. 2024;81:471–9.
https://doi.org/10.1136/oemed-2024-109621
.")\]. Analysis of PASC trajectories in the general population showed a decline in prevalence, especially during the first year after infection \[[15](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR15 "Ballouz T, Menges D, Anagnostopoulos A, Domenghino A, Aschmann HE, Frei A, et al. Recovery and symptom trajectories up to two years after SARS-CoV-2 infection: population based, longitudinal cohort study. BMJ. 2023;381:e074425.
https://doi.org/10.1136/bmj-2022-074425
. (British Medical Journal Publishing Group;)."), [19](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR19 "Bowe B, Xie Y, Al-Aly Z. Postacute sequelae of COVID-19 at 2 years. Nat Med. 2023;29:2347–57.
https://doi.org/10.1038/s41591-023-02521-2
."), [20](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR20 "Hurme A, Viinanen A, Teräsjärvi J, Jalkanen P, Feuth T, Löyttyniemi E, et al. Post-COVID-19 condition in prospective inpatient and outpatient cohorts. Sci Rep. 2025;15:6925.
https://doi.org/10.1038/s41598-025-90819-1
.")\]. Nevertheless, a substantial proportion of individuals (18–47%) continued to experience PASC symptoms two years post-infection \[[15](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR15 "Ballouz T, Menges D, Anagnostopoulos A, Domenghino A, Aschmann HE, Frei A, et al. Recovery and symptom trajectories up to two years after SARS-CoV-2 infection: population based, longitudinal cohort study. BMJ. 2023;381:e074425.
https://doi.org/10.1136/bmj-2022-074425
. (British Medical Journal Publishing Group;)."), [20](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR20 "Hurme A, Viinanen A, Teräsjärvi J, Jalkanen P, Feuth T, Löyttyniemi E, et al. Post-COVID-19 condition in prospective inpatient and outpatient cohorts. Sci Rep. 2025;15:6925.
https://doi.org/10.1038/s41598-025-90819-1
."), [21](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR21 "Pfrommer LR, Diexer S, Klee B, Massag J, Gottschick C, Purschke O, et al. Post-COVID recovery is faster after an infection with the SARS-CoV-2 Omicron variant: a population-based cohort study. Infection. 2025;53:657–65.
https://doi.org/10.1007/s15010-024-02438-z
.")\]. Thereafter, available data is limited, especially among HCWs, although recent studies indicate a relevant ongoing burden of disease \[[11](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR11 "Cai M, Xie Y, Topol EJ, Al-Aly Z. Three-year outcomes of post-acute sequelae of COVID-19. Nat Med. 2024;30:1564–73.
https://doi.org/10.1038/s41591-024-02987-8
."), [22](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR22 "Rahmati M, Udeh R, Kang J, Dolja‐Gore X, McEvoy M, Kazemi A, et al. Long‐term sequelae of COVID‐19: a systematic review and meta‐analysis of symptoms 3 years post‐SARS‐CoV‐2 infection. J Med Virol. 2025;97:e70429.
https://doi.org/10.1002/jmv.70429
."),[23](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR23 "Vallée G, Xi D, Avramovic G, O’Kelly B, Lambert JS. Evaluating the longitudinal physical and psychological health effects of persistent long Covid 3.5 years after infection. PLoS ONE. 2025;20:e0326790.
https://doi.org/10.1371/journal.pone.0326790
."),[24](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR24 "Gottlieb M, Yu H, Chen J, Spatz ES, Gentile NL, Geyer RE, et al. Differences in Long COVID severity by duration of illness, symptom evolution, and vaccination: a longitudinal cohort study from the INSPIRE group. Lancet Reg Health Am. 2025;44:101026.
https://doi.org/10.1016/j.lana.2025.101026
."),[25](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR25 "Ballouz T, Kerksieck P, Haile SR, Dressel H, Hämmig O, Bauer GF, et al. Work ability trajectories and sick leave in individuals with post COVID-19 condition: 3-year follow-up of a population-based cohort. Lancet Reg Health Eur. 2026;61:101536.
https://doi.org/10.1016/j.lanepe.2025.101536
.")\].
To guide post-COVID-19 care and occupational health strategies, this study aims to identify PASC-specific symptoms and to investigate the evolution of PASC symptoms in HCWs up to four years after aSCV2 infection. We also compare individuals with and without subjective LC in terms of PASC symptomatology and assess changes in subjective LC and the associated limitations in daily living over time, for a more comprehensive understanding of both the clinical and self-perceived long-term impact of COVID-19.
## Methods
### Setting and participants
In 2022, a longitudinal multicentre cohort involving HCWs from 14 institutions in northeastern Switzerland was launched. Employees aged ≥ 16 years of any work type, with or without direct patient contact, were eligible for inclusion and all participants provided electronic informed consent. The study protocol was approved by the Ethics Committee of Eastern Switzerland (\#2020–00502).
### Data collection
#### Serological testing
Serological testing for anti-spike (anti-S) and anti-nucleocapsid (anti-N) antibodies was performed in May/June 2022 in all participants to identify asymptomatic infections \[[26](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR26 "Kahlert CR, Persi R, Güsewell S, Egger T, Leal-Neto OB, Sumer J, et al. Non-occupational and occupational factors associated with specific SARS-CoV-2 antibodies among hospital workers – a multicentre cross-sectional study. Clin Microbiol Infect. 2021;27:1336–44.
https://doi.org/10.1016/j.cmi.2021.05.014
.")\]. The antibodies were measured using the Roche Elecsys electrochemiluminescence immunoassay (Roche Diagnostics, Rotkreuz, Switzerland).
#### Baseline survey
At baseline (September 2022), data were collected through an electronic baseline questionnaire including questions on personal health, occupational and non-occupational exposures, SARS-CoV-2 infection and vaccination history.
#### Follow-up surveys
Follow-up surveys were conducted approximately every 6 months (March to April 2023, October to November 2023, April to May 2024, October to November 2024). In those questionnaires, participants indicated the presence and duration of PASC-compatible symptoms as well as whether they suffer from LC (ongoing, resolved, never experienced). Additionally, SARS-CoV-2 infection and vaccination status were regularly updated.
### Definitions
#### Infection status
Participants were classified as aSCV2-infected if they reported a positive SARS-CoV-2 swab between February 2020 and January 2021 \[[27](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR27 "Federal Office of Public Health. Virus variants overview. [Internet]. [cited 2025 Apr 21].
https://www.covid19.admin.ch/en/epidemiologic/virus-variants
. Accessed 21 Apr 2025.")\]. Participants were assigned to the uninfected control group if they reported no previous SARS-CoV-2 infection and had a negative anti-N antibody result in June 2022. Thus, participants with a positive swab after January 2021 or positive anti-N antibody results in June 2022 were excluded, ensuring that only aSCV2-infected and uninfected participants were included, while individuals infected with later viral variants were not considered. Potential reinfections after the initial aSCV2 infection were not considered, as testing for SARS-CoV-2 was no longer recommended by the Swiss Federal Office of Public Health after February 2022, leading to incomplete detection of later infections \[[28](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR28 "Coronavirus: Key Decisions of the Federal Council [Internet]. [cited 2025 May 2].
https://www.uvek.admin.ch/uvek/de/home/uvek/coronavirus/wichtige-entscheide.html
. Accessed 2 May 2025.")\]. Validation of self-reported swab results with data from the division of occupational medicine (performed in the largest participating hospital) showed excellent concordance \[[29](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR29 "Kohler P, Güsewell S, Seneghini M, Egger T, Leal O, Brucher A, et al. Impact of baseline SARS-CoV-2 antibody status on syndromic surveillance and the risk of subsequent COVID-19—a prospective multicenter cohort study. BMC Med. 2021;19:270.
https://doi.org/10.1186/s12916-021-02144-9
.")\].
#### PASC symptoms
The 24 symptoms included in the surveys were selected based on national SARS-CoV-2 testing recommendations during the early phase of the pandemic. The symptoms were: Fatigue, Loss of Smell/Taste, Brain Fog, Joint Pain, Hair Loss, Headache, Chest Pain, Muscle Pain, Shortness of Breath, Dizziness, Cough, Burnout or Exhaustion, Runny Nose, Fever, Sneezing, Sore Throat, Abdominal Pain, Loss of Appetite/Nausea, Chills or Shivering, Red or Itchy Eyes, Erectile Dysfunction, Diarrhea, Menstrual Complaints and Rash. Testing for SARS-CoV-2 in individuals with compatible symptoms, using either rapid antigen tests or polymerase chain reaction, was recommended and later became mandatory for access to public institutions, including hospitals, in Switzerland. Symptoms that were described as chronic (i.e., longer than 7 days) and had emerged after the start of the COVID-19 pandemic were considered as PASC-related. Indications of symptoms that were either acute or chronic with onset before the pandemic were assigned as being non-PASC-compatible.
#### Subjective LC and functional limitations
Subjective LC was based on participants’ self-assessment; no further diagnostic criteria were applied. Those self-reporting LC were asked to grade their attributed functional limitations using the PCFS, a scale used to assess the needs for rehabilitation or recovery in COVID-19 patients. It differentiates: 0 = no functional limitations, 1 = symptoms without significant impact on daily life, 2 = slight limitations of usual activities, 3 = substantial restrictions with reduced everyday functioning, and 4 = severe limitations with dependence on assistance for activities of daily living \[[30](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR30 "Klok FA, Boon GJAM, Barco S, Endres M, Geelhoed JJM, Knauss S, et al. The Post-COVID-19 Functional Status scale: a tool to measure functional status over time after COVID-19. Eur Respir J. 2020;56:2001494.
https://doi.org/10.1183/13993003.01494-2020
.")\].
### Study design
The study design entailed a cross-sectional and a longitudinal analysis. In the cross-sectional analysis, PASC-specific symptoms were identified by comparing aSCV2-infected and uninfected individuals. In the longitudinal analysis, trajectories of symptoms, LC and PCFS were analyzed in aSCV2-infected participants that reported at least one PASC symptom at baseline (Fig. [1](https://link.springer.com/article/10.1007/s15010-026-02768-0#Fig1)).
**Fig. 1**
[](https://link.springer.com/article/10.1007/s15010-026-02768-0/figures/1)
Study Flow showing the process of enrolment and allocation to the different groups. N = Number of Participants, HCWs = Health Care Workers, LC = long COVID, PASC = Post-Acute COVID-19 Sequelae, aSCV2 = ancestral SARS-CoV-2
[Full size image](https://link.springer.com/article/10.1007/s15010-026-02768-0/figures/1)
### Statistical analysis
For the cross-sectional analysis, demographic and clinical characteristics between aSCV2-infected participants and the uninfected controls were compared using descriptive statistics. We calculated p-values using the Wilcoxon rank-sum test for continuous variables and the chi-square test or Fisher’s exact test for categorical variables. To distinguish PASC-specific symptoms from non-specific symptoms, the chi-square test was used; symptoms being significantly more common in the aSCV2 group were considered PASC-specific. Furthermore, baseline characteristics, symptom counts, and symptom prevalence were compared between participants with and without subjective LC using the same methods as described for aSCV2- and uninfected participants.
For the longitudinal analysis, we calculated the prevalence (for binary outcomes) and the median (for continuous outcomes) at every time point. Alluvial plots were used, where appropriate, to visualize how individuals move across categories over time. The independent effect of time on the number of symptoms and on the prevalence of the three most common symptoms (fatigue, brain fog and loss of smell/taste) was assessed using negative binomial (for symptom count) and logistic regression analysis (for symptoms). Time points were included as categorical and not as a continuous variable, as the effect of time was assumed to be non-linear. To account for repeated measurements, mixed-effects models with a random intercept for each individual were used. Adjusted incidence rate ratios (aIRR) from the negative binomial regression and adjusted odds ratios (aOR) from the logistic regression for the different time points, along with corresponding 95% confidence intervals (CI) were calculated. The models were adjusted for a priori defined covariates, namely age, sex, and Body-Mass-Index (BMI). To account for attrition bias, sensitivity analyses were performed: one restricted to participants with complete data across all surveys and another by adding the number of observed time points per participant to the negative binomial regression model. Spearman’s rank correlation was used to assess the association between baseline and last follow-up values of PCFS and total symptom count.
Statistical significance was set at a p-value of \< 0.05. All statistical analyses and figures were created using R version 4.4.2 (2024–10-31); descriptive statistics were performed using “gtsummary”, for regression analyses the package “lme4” was used and correlation analyses were carried out using Base R.
## Results
### Study population
Of 3,986 HCWs who completed the survey in September 2022, 1,027 (25.8%) were included in the baseline analysis (median age: 44 years; 80.6% women), of whom 456 (44.4%) were aSCV2-infected and 571 (55.6%) were uninfected controls. A total of 2,959 participants were excluded due to infections during later pandemic phases or incomplete baseline surveys (Fig. [1](https://link.springer.com/article/10.1007/s15010-026-02768-0#Fig1); Supplementary Material Table S1).
Compared to controls, aSCV2-infected participants were younger (median age 41 vs. 47 years, p \< 0.001), more frequently employed as nurses (59.4% vs. 37.5%, p \< 0.001) and had children under age 6 at home (13.6% vs. 9.3%, p = 0.029), while a smaller proportion were smokers (13.6% vs. 21.4%, p = 0.001) (Table [1](https://link.springer.com/article/10.1007/s15010-026-02768-0#Tab1)). The median time from the first positive SARS-CoV-2 test to the baseline survey was 18.5 months and 47.5 months to the last survey (Supplementary Material Table S2).
**Table 1 Characteristics of the aSCV2-Infected Group Compared with the Non-Infected Control Group at Baseline (09/2022)**
[Full size table](https://link.springer.com/article/10.1007/s15010-026-02768-0/tables/1)
### Identification of PASC-specific symptoms and subjective LC
Among 24 potential PASC symptoms, 13 symptoms were significantly more common in the aSCV2 group, with fatigue (22.8% in aSCV2-infected and 7.4% in controls), loss of smell/taste (11.4% and 0.4%), and brain fog (8.3% and 1.8%) being the most frequent (Fig. [2](https://link.springer.com/article/10.1007/s15010-026-02768-0#Fig2); Supplementary Material Table S3).
**Fig. 2**
[](https://link.springer.com/article/10.1007/s15010-026-02768-0/figures/2)
Absolute difference in symptom prevalence (%) between the ancestral SARS CoV-2 (aSCV2) infected group and the non-infected control group at baseline (09/2022) represented as dots, with 95% confidence intervals. Orange = PASC-specific symptoms; blue = non-specific symptoms
[Full size image](https://link.springer.com/article/10.1007/s15010-026-02768-0/figures/2)
Among HCWs with PASC-specific symptoms at baseline (n = 186/1027, 18.1%), 38% (n = 70) self-reported having LC, while 62% (n = 116) did not (anymore). Participants with subjective LC at baseline had a higher median number of symptoms compared to those without subjective LC (4 vs 1) (Table S4).
### Trajectory of symptoms
Out of 456 aSCV2-infected participants, 40.8% (n = 186) reported at least one PASC-specific symptom and were included in the longitudinal analysis. Participants completed a median of 3 surveys (range 1–5). Overall, 72.0% (n = 134) did not have complete data or were lost to follow-up during the course of the study. Compared to those with complete data, these participants were younger (median age 39 vs. 47.5 years), more often male (14.9% vs. 23.1%), more commonly smokers (11.9% vs. 5.8%) and more frequently working full-time (45.5% vs. 34.6%). Additionally, they were less likely to report comorbidities other than pollen allergy (33.3% vs. 58.6%) (Supplementary Material Table S5).
The median number of symptoms declined from 2 at baseline to 0 symptoms in the last survey, and from 2 to 1 in participants with complete data (n = 52); the decline was most pronounced from the baseline to the first follow-up survey and remained mostly stable thereafter (Fig. [3](https://link.springer.com/article/10.1007/s15010-026-02768-0#Fig3); Supplementary Material Table S6). In the last survey (median 47.5 months after infection), 58.6% of all participants (59.6% of participants with complete data) still reported ≥ 1 PASC symptom, with fatigue being the most persistent symptom (35.7%) (Supplementary Material Table S7/ Table S8). For those with complete data, participants with an initially high number of symptoms tended to also have higher symptom scores in the last survey (Spearman’s ρ = 0.338, p = 0.014) (Fig. [3](https://link.springer.com/article/10.1007/s15010-026-02768-0#Fig3); Supplementary Material Figure S1).
**Fig. 3**
[](https://link.springer.com/article/10.1007/s15010-026-02768-0/figures/3)
**A** displays the count of symptoms for each time point, grouped as described in the legend, for all participants including participants that dropped out (n=186). The dashed black line and error bars represent the adjusted incidence rate ratio (aIRR) and 95% confidence intervals for symptom count, referenced to baseline (09/2022). **B** shows longitudinal trajectories of symptom groups among participants with complete data at every time point (n=52), with the black solid line indicating the median number of symptoms at each time point
[Full size image](https://link.springer.com/article/10.1007/s15010-026-02768-0/figures/3)
Assessment of symptom trajectories using the negative binomial mixed-effects model showed a significant decline in the number of symptoms per participant at the last survey compared to baseline (aIRR 0.71, 95% CI 0.58–0.87, p = 0.001). Results were similar with complete case analysis (aIRR = 0.72, 95% CI 0.56–0.93, p = 0.013) (Supplementary Material Table S9).
For the three most prevalent symptoms, fatigue decreased from 55.9% (104/186) to 35.7% (25/70) (aOR 0.23, 95% CI 0.10–0.52, p \< 0.001), loss of smell/taste from 28.0% (52/186) to 18.6% (13/70) (aOR 0.03, 95% CI 0.00–0.21, p \< 0.001) and brain fog changed from 20.4% (38/186) to 14.3% (10/70) without being significant (aOR 0.96, 95% CI 0.27–3.37, p = 0.95) (Fig. [4](https://link.springer.com/article/10.1007/s15010-026-02768-0#Fig4)). Figures were similar in the subset of participants with complete data (Supplementary Material Figure S2; Table S10).
**Fig. 4**
[](https://link.springer.com/article/10.1007/s15010-026-02768-0/figures/4)
Bar graphs showing the prevalence of the three most prevalent PASC-specific symptoms (Fatigue, Brain Fog, Loss of Smell/ Taste) in participants with available data at each follow-up time point. The black line shows the adjusted Odds Ratio (aOR) with 95% confidence intervals for symptom presence at each time point (relative to baseline), shown as error bars. Sample size: 09/2022: n=186, 03/2023: n=124, 10/2023: n=105, 04/2024: n=83, 10/2024: n=70
[Full size image](https://link.springer.com/article/10.1007/s15010-026-02768-0/figures/4)
### Trajectory of subjective LC and functional status
77 of the 456 aSCV2-infected participants reported LC at baseline. To ensure consistency with the longitudinal symptom trajectory analyses, only participants reporting ≥ 1 PASC-specific chronic symptom were included. In this subgroup, 70 of 186 individuals reported subjective LC, of whom 12.9% (9/70) reported resolution of symptoms at the first follow-up. Thereafter, there were no new reports of resolved symptoms. At the final follow-up, only 18 of the initial 70 participants remained, with 14 indicating ongoing subjective LC (Supplementary Material Figure S3; Table S11).
When analyzing the PCFS score at baseline, 71.4% (n = 50) of participants with subjective LC had no or minor (PCFS 0 or 1) limitations in their daily life. This figure remained stable over time as did the median PCFS. Participants with moderate or severe limitations (PCFS score ≥ 2) at baseline tended to still report limitations at the final follow-up (Spearman’s ρ = 0.40, p = 0.10). However, data availability declined over follow-up due to decreasing subjective LC reports and participant attrition (Supplementary Material Figures S4, S5; Table S12).
## Discussion
In a prospective multicentre cohort of HCWs, we demonstrate a non-linear decline in PASC-specific symptoms over time, with up to 60% of individuals still reporting symptoms after a median of almost 4 years after aSCV2 infection. Fatigue, brain fog, and loss of smell or taste are the most prevalent symptoms. For those with subjective LC, the limitations in daily life are mostly mild, but often persist over time.
The prevalence of PASC symptoms at baseline was 40.8% (median 18.5 months post-infection), which is higher than reported in prior studies \[[15](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR15 "Ballouz T, Menges D, Anagnostopoulos A, Domenghino A, Aschmann HE, Frei A, et al. Recovery and symptom trajectories up to two years after SARS-CoV-2 infection: population based, longitudinal cohort study. BMJ. 2023;381:e074425.
https://doi.org/10.1136/bmj-2022-074425
. (British Medical Journal Publishing Group;)."), [31](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR31 "Fernandez-de-las-Peñas C, Notarte KI, Macasaet R, Velasco JV, Catahay JA, Ver AT, et al. Persistence of post-COVID symptoms in the general population two years after SARS-CoV-2 infection: a systematic review and meta-analysis. J Infect. 2024;88:77–88.
https://doi.org/10.1016/j.jinf.2023.12.004
."), [32](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR32 "Kim Y, Bae S, Chang H-H, Kim S-W. Long COVID prevalence and impact on quality of life 2 years after acute COVID-19. Sci Rep. 2023;13:11207.
https://doi.org/10.1038/s41598-023-36995-4
.")\]. A recent meta-analysis including only studies with more than 3 years of follow-up, showed a pooled prevalence of 20% at 3 years, again lower than our findings (67% at 3 years). However, the individual studies contributing to this analysis showed a wide range of prevalence estimates (6–54%) \[[22](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR22 "Rahmati M, Udeh R, Kang J, Dolja‐Gore X, McEvoy M, Kazemi A, et al. Long‐term sequelae of COVID‐19: a systematic review and meta‐analysis of symptoms 3 years post‐SARS‐CoV‐2 infection. J Med Virol. 2025;97:e70429.
https://doi.org/10.1002/jmv.70429
.")\]. One factor for this difference could be the high exposure of our cohort during the aSCV2 period compared to non-HCWs, as this viral variant was shown to have the highest PASC incidence one year post-infection, with declining rates observed for later variants \[[8](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR8 "Xie Y, Choi T, Al-Aly Z. Postacute sequelae of SARS-CoV-2 infection in the Pre-Delta, Delta, and Omicron eras. N Engl J Med. 2024;391:515–25.
https://doi.org/10.1056/NEJMoa2403211
.")\]. Consistent with previous reports of neurological symptoms persisting, brain fog showed no significant decline, suggesting ongoing cognitive impairment in PASC affected patients \[[15](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR15 "Ballouz T, Menges D, Anagnostopoulos A, Domenghino A, Aschmann HE, Frei A, et al. Recovery and symptom trajectories up to two years after SARS-CoV-2 infection: population based, longitudinal cohort study. BMJ. 2023;381:e074425.
https://doi.org/10.1136/bmj-2022-074425
. (British Medical Journal Publishing Group;)."), [33](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR33 "Nguyen NN, Tissot-Dupont H, Brouqui P, Gautret P. Post-COVID syndrome in symptomatic COVID-19 patients: a retrospective cohort study. BMC Infect Dis. 2025;25:1099.
https://doi.org/10.1186/s12879-025-11360-0
.")\].
In our cohort, self-reported LC was associated with a higher number of symptoms and specific symptoms, most notably fatigue (80% vs. 41% without LC), which is in line with previous findings \[[34](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR34 "Danesh V, Arroliga AC, Bourgeois JA, Boehm LM, McNeal MJ, Widmer AJ, et al. Symptom clusters seen in adult COVID-19 recovery clinic care seekers. J Gen Intern Med. 2023;38:442–9.
https://doi.org/10.1007/s11606-022-07908-4
."),[35](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR35 "Huiberts AJ, De Bruijn S, Andeweg SP, Hoeve CE, Schipper M, De Melker HE, et al. Prospective cohort study of fatigue before and after SARS-CoV-2 infection in the Netherlands. Nat Commun. 2025;16:1923.
https://doi.org/10.1038/s41467-025-56994-5
."),[36](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR36 "Strahm C, Seneghini M, Güsewell S, Egger T, Leal-Neto O, Brucher A, et al. Symptoms compatible with long coronavirus disease (COVID) in healthcare workers with and without severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection—results of a prospective multicenter cohort. Clin Infect Dis. 2022;75:e1011–9.
https://doi.org/10.1093/cid/ciac054
.")\]. Gottlieb et al. had a similar design with self-reported LC through continuous surveys. In a cross-sectional analysis up to 40 months post-infection, only 2% reported resolved LC and only 26% of participants with current LC reported improved symptoms \[[24](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR24 "Gottlieb M, Yu H, Chen J, Spatz ES, Gentile NL, Geyer RE, et al. Differences in Long COVID severity by duration of illness, symptom evolution, and vaccination: a longitudinal cohort study from the INSPIRE group. Lancet Reg Health Am. 2025;44:101026.
https://doi.org/10.1016/j.lana.2025.101026
.")\]. This persistence of LC is consistent with our analysis of subjective LC prevalence, where no participants reported resolved symptoms after the first follow-up and the trend in functional limitations (PCFS), where only a small subset reported complete resolution of limitations.
Our findings indicate that full recovery from PASC remains uncertain for many patients and functional limitations persist. PASC should be recognized as a chronic condition requiring long-term clinical and social support, and further research has to be supported to clarify the pathophysiology and to identify diagnostic markers and effective treatment. As our cohort consists of HCWs, these findings underline the need for occupational health strategies, including structured return-to-work programs and flexible workload adjustments, to support sustainable reintegration and minimize the loss of essential workforce.
### Limitations
This study has several limitations. First, prior infection status was partially based on anti-N antibody negativity. We acknowledge that some previously infected individuals may have been misclassified due to absent seroconversion or declining antibody levels over time, which may have led to misclassification in the cross-sectional analysis and to over- or underestimation of symptom prevalence across time points \[[37](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR37 "Nakagama Y, Komase Y, Kaku N, Nitahara Y, Tshibangu-Kabamba E, Tominaga T, et al. Detecting waning serological response with commercial immunoassays: 18-month longitudinal follow-up of anti-SARS-CoV-2 Nucleocapsid antibodies. Microbiol Spectr. 2022;10:e00986-22.
https://doi.org/10.1128/spectrum.00986-22
.")\]. To minimize this risk, we not only required anti-N negativity for classification into the uninfected control group, but also the absence of a documented positive SARS-CoV-2 test. Given the extensive and partly mandatory testing policies for HCWs until February 2022, we consider the likelihood of undetected infections in our cohort to be low.
Second, information bias due to self-reported data may have caused misclassification and over- or underestimation of prevalence rates.
Third, substantial loss to follow-up limited the size of the dataset and potentially introduced attrition bias, causing an underestimation of PASC-prevalence if affected participants were less likely to remain in the study. However, sensitivity analyses focusing on participants with complete data and a model adjusted for the number of answered surveys mostly confirmed our results. Although regression models were adjusted for age, sex, and BMI, residual confounding by unmeasured factors, such as pre-existing comorbidities, mental health status, or occupational stress is possible. These factors may have influenced both the likelihood of infection and the reporting of persistent symptoms, potentially leading to over- or underestimation of the observed outcomes. In addition, effect modification by baseline health status or pre-existing comorbidities cannot be ruled out.
Fourth, survivor bias cannot be excluded. Only individuals who survived aSCV2 infection and remained in the workforce until 2022 were eligible for inclusion. Individuals who experienced severe outcomes, left the workforce due to functional impairment, or died were not captured, which may have led to an underestimation of the true long-term burden of PASC.
Fifth, reinfections were not assessed, as mandatory SARS-CoV-2 testing in Switzerland was discontinued in February 2022; undetected reinfections may therefore have biased symptom trajectories \[[28](https://link.springer.com/article/10.1007/s15010-026-02768-0#ref-CR28 "Coronavirus: Key Decisions of the Federal Council [Internet]. [cited 2025 May 2].
https://www.uvek.admin.ch/uvek/de/home/uvek/coronavirus/wichtige-entscheide.html
. Accessed 2 May 2025.")\].
Finally, the transferability of our findings to the general population is limited, as HCWs may differ in exposure risk and health-seeking behavior.
Strengths of this study include clearly defined infection groups through serology and timing, and a unique follow-up period providing data up to four years post-infection. Furthermore, PCFS scoring allowed assessment of functional limitations over time.
This study provides four-year follow-up data on PASC in a predominantly young and healthy cohort. Despite a general decline in symptom prevalence, key symptoms such as fatigue, brain fog, and loss of smell or taste persisted in a substantial subset up to four years post-aSCV2 infection. Long-term follow-up and tailored care strategies appear essential for managing persistent PASC symptoms.
## Data availability
All data generated or analysed during this study are included in this published article and its Supplementary Material.
## References
1. Post COVID-19 condition (Long COVID) \[Internet\]. <https://www.who.int/europe/news-room/fact-sheets/item/post-covid-19-condition>. Accessed 15 Jan 2025.
2. Parums DV. Long COVID or Post-Acute Sequelae of SARS-CoV-2 Infection (PASC) and the urgent need to identify diagnostic biomarkers and risk factors. Med Sci Monit. 2024. <https://doi.org/10.12659/MSM.946512>.
[Article](https://doi.org/10.12659%2FMSM.946512) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=39616449) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC11619173) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Long%20COVID%20or%20Post-Acute%20Sequelae%20of%20SARS-CoV-2%20Infection%20%28PASC%29%20and%20the%20urgent%20need%20to%20identify%20diagnostic%20biomarkers%20and%20risk%20factors&journal=Med%20Sci%20Monit&doi=10.12659%2FMSM.946512&publication_year=2024&author=Parums%2CDV)
3. Davis HE, McCorkell L, Vogel JM, Topol EJ. Long COVID: major findings, mechanisms and recommendations. Nat Rev Microbiol. 2023;21:133–46. <https://doi.org/10.1038/s41579-022-00846-2>.
[Article](https://doi.org/10.1038%2Fs41579-022-00846-2) [CAS](https://link.springer.com/articles/cas-redirect/1:CAS:528:DC%2BB3sXhtV2rtrw%3D) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=36639608) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC9839201) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Long%20COVID%3A%20major%20findings%2C%20mechanisms%20and%20recommendations&journal=Nat%20Rev%20Microbiol&doi=10.1038%2Fs41579-022-00846-2&volume=21&pages=133-146&publication_year=2023&author=Davis%2CHE&author=McCorkell%2CL&author=Vogel%2CJM&author=Topol%2CEJ)
4. Reese JT, Blau H, Casiraghi E, Bergquist T, Loomba JJ, Callahan TJ, et al. Generalisable long COVID subtypes: findings from the NIH N3C and RECOVER programmes. EBioMedicine. 2023;87:104413. <https://doi.org/10.1016/j.ebiom.2022.104413>.
[Article](https://doi.org/10.1016%2Fj.ebiom.2022.104413) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=36563487) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Generalisable%20long%20COVID%20subtypes%3A%20findings%20from%20the%20NIH%20N3C%20and%20RECOVER%20programmes&journal=EBioMedicine&doi=10.1016%2Fj.ebiom.2022.104413&volume=87&publication_year=2023&author=Reese%2CJT&author=Blau%2CH&author=Casiraghi%2CE&author=Bergquist%2CT&author=Loomba%2CJJ&author=Callahan%2CTJ)
5. Thaweethai T, Jolley SE, Karlson EW, Levitan EB, Levy B, McComsey GA, et al. Development of a definition of postacute sequelae of SARS-CoV-2 infection. JAMA. 2023;329:1934. <https://doi.org/10.1001/jama.2023.8823>.
[Article](https://doi.org/10.1001%2Fjama.2023.8823) [CAS](https://link.springer.com/articles/cas-redirect/1:CAS:528:DC%2BB3sXht1KqtL%2FL) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=37278994) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC10214179) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Development%20of%20a%20definition%20of%20postacute%20sequelae%20of%20SARS-CoV-2%20infection&journal=JAMA&doi=10.1001%2Fjama.2023.8823&volume=329&publication_year=2023&author=Thaweethai%2CT&author=Jolley%2CSE&author=Karlson%2CEW&author=Levitan%2CEB&author=Levy%2CB&author=McComsey%2CGA)
6. Griffin DO. Postacute sequelae of COVID (PASC or Long COVID): an evidenced-based approach. Open Forum Infect Dis. 2024;11:ofae462. <https://doi.org/10.1093/ofid/ofae462>.
[Article](https://doi.org/10.1093%2Fofid%2Fofae462) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=39220656) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC11363684) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Postacute%20sequelae%20of%20COVID%20%28PASC%20or%20Long%20COVID%29%3A%20an%20evidenced-based%20approach&journal=Open%20Forum%20Infect%20Dis&doi=10.1093%2Fofid%2Fofae462&volume=11&publication_year=2024&author=Griffin%2CDO)
7. Hastie CE, Lowe DJ, McAuley A, Mills NL, Winter AJ, Black C, et al. True prevalence of long-COVID in a nationwide, population cohort study. Nat Commun. 2023;14:7892. <https://doi.org/10.1038/s41467-023-43661-w>.
[Article](https://doi.org/10.1038%2Fs41467-023-43661-w) [CAS](https://link.springer.com/articles/cas-redirect/1:CAS:528:DC%2BB3sXisFSls7rP) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=38036541) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC10689486) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=True%20prevalence%20of%20long-COVID%20in%20a%20nationwide%2C%20population%20cohort%20study&journal=Nat%20Commun&doi=10.1038%2Fs41467-023-43661-w&volume=14&publication_year=2023&author=Hastie%2CCE&author=Lowe%2CDJ&author=McAuley%2CA&author=Mills%2CNL&author=Winter%2CAJ&author=Black%2CC)
8. Xie Y, Choi T, Al-Aly Z. Postacute sequelae of SARS-CoV-2 infection in the Pre-Delta, Delta, and Omicron eras. N Engl J Med. 2024;391:515–25. <https://doi.org/10.1056/NEJMoa2403211>.
[Article](https://doi.org/10.1056%2FNEJMoa2403211) [CAS](https://link.springer.com/articles/cas-redirect/1:CAS:528:DC%2BB2cXhvVCqs7fN) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=39018527) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC11687648) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Postacute%20sequelae%20of%20SARS-CoV-2%20infection%20in%20the%20Pre-Delta%2C%20Delta%2C%20and%20Omicron%20eras&journal=N%20Engl%20J%20Med&doi=10.1056%2FNEJMoa2403211&volume=391&pages=515-525&publication_year=2024&author=Xie%2CY&author=Choi%2CT&author=Al-Aly%2CZ)
9. Sherif ZA, Gomez CR, Connors TJ, Henrich TJ, Reeves WB, RECOVER Mechanistic Pathway Task Force. Pathogenic mechanisms of post-acute sequelae of SARS-CoV-2 infection (PASC). Elife. 2023;12:e86002. <https://doi.org/10.7554/eLife.86002>.
[Article](https://doi.org/10.7554%2FeLife.86002) [CAS](https://link.springer.com/articles/cas-redirect/1:CAS:528:DC%2BB2cXmtFans7c%3D) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=36947108) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC10032659) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Pathogenic%20mechanisms%20of%20post-acute%20sequelae%20of%20SARS-CoV-2%20infection%20%28PASC%29&journal=Elife&doi=10.7554%2FeLife.86002&volume=12&publication_year=2023&author=Sherif%2CZA&author=Gomez%2CCR&author=Connors%2CTJ&author=Henrich%2CTJ&author=Reeves%2CWB)
10. Mandel H, Yoo YJ, Allen AJ, Abedian S, Verzani Z, Karlson EW, et al. Long COVID incidence proportion in adults and children between 2020 and 2024: an EHR-based study from the RECOVER initiative. Clin Infect Dis. 2025. <https://doi.org/10.1093/cid/ciaf046>.
[Article](https://doi.org/10.1093%2Fcid%2Fciaf046) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=39907495) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC12272849) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Long%20COVID%20incidence%20proportion%20in%20adults%20and%20children%20between%202020%20and%202024%3A%20an%20EHR-based%20study%20from%20the%20RECOVER%20initiative&journal=Clin%20Infect%20Dis&doi=10.1093%2Fcid%2Fciaf046&publication_year=2025&author=Mandel%2CH&author=Yoo%2CYJ&author=Allen%2CAJ&author=Abedian%2CS&author=Verzani%2CZ&author=Karlson%2CEW)
11. Cai M, Xie Y, Topol EJ, Al-Aly Z. Three-year outcomes of post-acute sequelae of COVID-19. Nat Med. 2024;30:1564–73. <https://doi.org/10.1038/s41591-024-02987-8>.
[Article](https://doi.org/10.1038%2Fs41591-024-02987-8) [CAS](https://link.springer.com/articles/cas-redirect/1:CAS:528:DC%2BB2cXht1yhsLvJ) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=38816608) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC11186764) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Three-year%20outcomes%20of%20post-acute%20sequelae%20of%20COVID-19&journal=Nat%20Med&doi=10.1038%2Fs41591-024-02987-8&volume=30&pages=1564-1573&publication_year=2024&author=Cai%2CM&author=Xie%2CY&author=Topol%2CEJ&author=Al-Aly%2CZ)
12. Groff D, Sun A, Ssentongo AE, Ba DM, Parsons N, Poudel GR, et al. Short-term and long-term rates of postacute sequelae of SARS-CoV-2 infection: a systematic review. JAMA Netw Open. 2021;4:e2128568. <https://doi.org/10.1001/jamanetworkopen.2021.28568>.
[Article](https://doi.org/10.1001%2Fjamanetworkopen.2021.28568) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=34643720) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC8515212) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Short-term%20and%20long-term%20rates%20of%20postacute%20sequelae%20of%20SARS-CoV-2%20infection%3A%20a%20systematic%20review&journal=JAMA%20Netw%20Open&doi=10.1001%2Fjamanetworkopen.2021.28568&volume=4&publication_year=2021&author=Groff%2CD&author=Sun%2CA&author=Ssentongo%2CAE&author=Ba%2CDM&author=Parsons%2CN&author=Poudel%2CGR)
13. Kahlert CR, Strahm C, Güsewell S, Cusini A, Brucher A, Goppel S, et al. Post-acute sequelae after Severe Acute Respiratory Syndrome Coronavirus 2 infection by viral variant and vaccination status: a multicenter cross-sectional study. Clin Infect Dis. 2023;77:194–202. <https://doi.org/10.1093/cid/ciad143>.
[Article](https://doi.org/10.1093%2Fcid%2Fciad143) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=36905145) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC10371307) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Post-acute%20sequelae%20after%20Severe%20Acute%20Respiratory%20Syndrome%20Coronavirus%202%20infection%20by%20viral%20variant%20and%20vaccination%20status%3A%20a%20multicenter%20cross-sectional%20study&journal=Clin%20Infect%20Dis&doi=10.1093%2Fcid%2Fciad143&volume=77&pages=194-202&publication_year=2023&author=Kahlert%2CCR&author=Strahm%2CC&author=G%C3%BCsewell%2CS&author=Cusini%2CA&author=Brucher%2CA&author=Goppel%2CS)
14. Dörr T, Strahm C, Güsewell S, Ballouz T, Kocan E, Cusini A, et al. Burden of post–acute COVID-19 sequelae in healthcare workers and its course over a 30-month period–results from a prospective multicentre cohort. Infection. 2024. <https://doi.org/10.1007/s15010-024-02418-3>.
[Article](https://link.springer.com/doi/10.1007/s15010-024-02418-3) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=39532773) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC12316709) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Burden%20of%20post%E2%80%93acute%20COVID-19%20sequelae%20in%20healthcare%20workers%20and%20its%20course%20over%20a%2030-month%20period%E2%80%93results%20from%20a%20prospective%20multicentre%20cohort&journal=Infection&doi=10.1007%2Fs15010-024-02418-3&publication_year=2024&author=D%C3%B6rr%2CT&author=Strahm%2CC&author=G%C3%BCsewell%2CS&author=Ballouz%2CT&author=Kocan%2CE&author=Cusini%2CA)
15. Ballouz T, Menges D, Anagnostopoulos A, Domenghino A, Aschmann HE, Frei A, et al. Recovery and symptom trajectories up to two years after SARS-CoV-2 infection: population based, longitudinal cohort study. BMJ. 2023;381:e074425. <https://doi.org/10.1136/bmj-2022-074425>. (**British Medical Journal Publishing Group;**).
[Article](https://doi.org/10.1136%2Fbmj-2022-074425) [CAS](https://link.springer.com/articles/cas-redirect/1:CAS:528:DC%2BB2MXlt12ktbk%3D) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=37257891) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC10230608) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Recovery%20and%20symptom%20trajectories%20up%20to%20two%20years%20after%20SARS-CoV-2%20infection%3A%20population%20based%2C%20longitudinal%20cohort%20study&journal=BMJ&doi=10.1136%2Fbmj-2022-074425&volume=381&publication_year=2023&author=Ballouz%2CT&author=Menges%2CD&author=Anagnostopoulos%2CA&author=Domenghino%2CA&author=Aschmann%2CHE&author=Frei%2CA)
16. Foulkes S, Evans J, Neill C, Bishop J, Khawam J, Islam J, et al. Prevalence and impact of persistent symptoms following SARS-CoV-2 infection among healthcare workers: a cross-sectional survey in the SIREN cohort. J Infect. 2024;89:106259. <https://doi.org/10.1016/j.jinf.2024.106259>.
[Article](https://doi.org/10.1016%2Fj.jinf.2024.106259) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=39214242) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Prevalence%20and%20impact%20of%20persistent%20symptoms%20following%20SARS-CoV-2%20infection%20among%20healthcare%20workers%3A%20a%20cross-sectional%20survey%20in%20the%20SIREN%20cohort&journal=J%20Infect&doi=10.1016%2Fj.jinf.2024.106259&volume=89&publication_year=2024&author=Foulkes%2CS&author=Evans%2CJ&author=Neill%2CC&author=Bishop%2CJ&author=Khawam%2CJ&author=Islam%2CJ)
17. Lim SH, Lim YC, Zaki RA, Johari BM, Chang CY, Omar SFS, et al. Prevalence and predictors of post-acute COVID syndrome among infected healthcare workers at University Malaya Medical Centre. PLoS ONE. 2024;19:e0298376. <https://doi.org/10.1371/journal.pone.0298376>.
[Article](https://doi.org/10.1371%2Fjournal.pone.0298376) [CAS](https://link.springer.com/articles/cas-redirect/1:CAS:528:DC%2BB2cXpsVOqsr0%3D) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=38626017) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC11020391) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Prevalence%20and%20predictors%20of%20post-acute%20COVID%20syndrome%20among%20infected%20healthcare%20workers%20at%20University%20Malaya%20Medical%20Centre&journal=PLoS%20ONE&doi=10.1371%2Fjournal.pone.0298376&volume=19&publication_year=2024&author=Lim%2CSH&author=Lim%2CYC&author=Zaki%2CRA&author=Johari%2CBM&author=Chang%2CCY&author=Omar%2CSFS)
18. Dempsey B, Blake HA, Madan I, Stevelink SAM, Greenberg N, Raine R, et al. Post COVID-19 syndrome among 5248 healthcare workers in England: longitudinal findings from NHS CHECK. Occup Environ Med. 2024;81:471–9. <https://doi.org/10.1136/oemed-2024-109621>.
[Article](https://doi.org/10.1136%2Foemed-2024-109621) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=39358009) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC11503206) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Post%20COVID-19%20syndrome%20among%205248%20healthcare%20workers%20in%20England%3A%20longitudinal%20findings%20from%20NHS%20CHECK&journal=Occup%20Environ%20Med&doi=10.1136%2Foemed-2024-109621&volume=81&pages=471-479&publication_year=2024&author=Dempsey%2CB&author=Blake%2CHA&author=Madan%2CI&author=Stevelink%2CSAM&author=Greenberg%2CN&author=Raine%2CR)
19. Bowe B, Xie Y, Al-Aly Z. Postacute sequelae of COVID-19 at 2 years. Nat Med. 2023;29:2347–57. <https://doi.org/10.1038/s41591-023-02521-2>.
[Article](https://doi.org/10.1038%2Fs41591-023-02521-2) [CAS](https://link.springer.com/articles/cas-redirect/1:CAS:528:DC%2BB3sXhslektrrL) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=37605079) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC10504070) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Postacute%20sequelae%20of%20COVID-19%20at%202%20years&journal=Nat%20Med&doi=10.1038%2Fs41591-023-02521-2&volume=29&pages=2347-2357&publication_year=2023&author=Bowe%2CB&author=Xie%2CY&author=Al-Aly%2CZ)
20. Hurme A, Viinanen A, Teräsjärvi J, Jalkanen P, Feuth T, Löyttyniemi E, et al. Post-COVID-19 condition in prospective inpatient and outpatient cohorts. Sci Rep. 2025;15:6925. <https://doi.org/10.1038/s41598-025-90819-1>.
[Article](https://doi.org/10.1038%2Fs41598-025-90819-1) [CAS](https://link.springer.com/articles/cas-redirect/1:CAS:528:DC%2BB2MXlt1Wkt74%3D) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=40011519) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC11865615) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Post-COVID-19%20condition%20in%20prospective%20inpatient%20and%20outpatient%20cohorts&journal=Sci%20Rep&doi=10.1038%2Fs41598-025-90819-1&volume=15&publication_year=2025&author=Hurme%2CA&author=Viinanen%2CA&author=Ter%C3%A4sj%C3%A4rvi%2CJ&author=Jalkanen%2CP&author=Feuth%2CT&author=L%C3%B6yttyniemi%2CE)
21. Pfrommer LR, Diexer S, Klee B, Massag J, Gottschick C, Purschke O, et al. Post-COVID recovery is faster after an infection with the SARS-CoV-2 Omicron variant: a population-based cohort study. Infection. 2025;53:657–65. <https://doi.org/10.1007/s15010-024-02438-z>.
[Article](https://link.springer.com/doi/10.1007/s15010-024-02438-z) [CAS](https://link.springer.com/articles/cas-redirect/1:CAS:528:DC%2BB2cXisF2ntL3O) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=39556163) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Post-COVID%20recovery%20is%20faster%20after%20an%20infection%20with%20the%20SARS-CoV-2%20Omicron%20variant%3A%20a%20population-based%20cohort%20study&journal=Infection&doi=10.1007%2Fs15010-024-02438-z&volume=53&pages=657-665&publication_year=2025&author=Pfrommer%2CLR&author=Diexer%2CS&author=Klee%2CB&author=Massag%2CJ&author=Gottschick%2CC&author=Purschke%2CO)
22. Rahmati M, Udeh R, Kang J, Dolja‐Gore X, McEvoy M, Kazemi A, et al. Long‐term sequelae of COVID‐19: a systematic review and meta‐analysis of symptoms 3 years post‐SARS‐CoV‐2 infection. J Med Virol. 2025;97:e70429. <https://doi.org/10.1002/jmv.70429>.
[Article](https://doi.org/10.1002%2Fjmv.70429) [CAS](https://link.springer.com/articles/cas-redirect/1:CAS:528:DC%2BB2MXhtlKgsrfM) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=40476637) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC12143191) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Long%E2%80%90term%20sequelae%20of%20COVID%E2%80%9019%3A%20a%20systematic%20review%20and%20meta%E2%80%90analysis%20of%20symptoms%203%20years%20post%E2%80%90SARS%E2%80%90CoV%E2%80%902%20infection&journal=J%20Med%20Virol&doi=10.1002%2Fjmv.70429&volume=97&publication_year=2025&author=Rahmati%2CM&author=Udeh%2CR&author=Kang%2CJ&author=Dolja%E2%80%90Gore%2CX&author=McEvoy%2CM&author=Kazemi%2CA)
23. Vallée G, Xi D, Avramovic G, O’Kelly B, Lambert JS. Evaluating the longitudinal physical and psychological health effects of persistent long Covid 3.5 years after infection. PLoS ONE. 2025;20:e0326790. <https://doi.org/10.1371/journal.pone.0326790>.
[Article](https://doi.org/10.1371%2Fjournal.pone.0326790) [CAS](https://link.springer.com/articles/cas-redirect/1:CAS:528:DC%2BB2MXhsFemtb7P) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=40554575) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC12186912) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Evaluating%20the%20longitudinal%20physical%20and%20psychological%20health%20effects%20of%20persistent%20long%20Covid%203.5%20years%20after%20infection&journal=PLoS%20ONE&doi=10.1371%2Fjournal.pone.0326790&volume=20&publication_year=2025&author=Vall%C3%A9e%2CG&author=Xi%2CD&author=Avramovic%2CG&author=O%E2%80%99Kelly%2CB&author=Lambert%2CJS)
24. Gottlieb M, Yu H, Chen J, Spatz ES, Gentile NL, Geyer RE, et al. Differences in Long COVID severity by duration of illness, symptom evolution, and vaccination: a longitudinal cohort study from the INSPIRE group. Lancet Reg Health Am. 2025;44:101026. <https://doi.org/10.1016/j.lana.2025.101026>.
[Article](https://doi.org/10.1016%2Fj.lana.2025.101026) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=40040820) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC11875141) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Differences%20in%20Long%20COVID%20severity%20by%20duration%20of%20illness%2C%20symptom%20evolution%2C%20and%20vaccination%3A%20a%20longitudinal%20cohort%20study%20from%20the%20INSPIRE%20group&journal=Lancet%20Reg%20Health%20Am&doi=10.1016%2Fj.lana.2025.101026&volume=44&publication_year=2025&author=Gottlieb%2CM&author=Yu%2CH&author=Chen%2CJ&author=Spatz%2CES&author=Gentile%2CNL&author=Geyer%2CRE)
25. Ballouz T, Kerksieck P, Haile SR, Dressel H, Hämmig O, Bauer GF, et al. Work ability trajectories and sick leave in individuals with post COVID-19 condition: 3-year follow-up of a population-based cohort. Lancet Reg Health Eur. 2026;61:101536. <https://doi.org/10.1016/j.lanepe.2025.101536>.
[Article](https://doi.org/10.1016%2Fj.lanepe.2025.101536) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=41362299) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Work%20ability%20trajectories%20and%20sick%20leave%20in%20individuals%20with%20post%20COVID-19%20condition%3A%203-year%20follow-up%20of%20a%20population-based%20cohort&journal=Lancet%20Reg%20Health%20Eur&doi=10.1016%2Fj.lanepe.2025.101536&volume=61&publication_year=2026&author=Ballouz%2CT&author=Kerksieck%2CP&author=Haile%2CSR&author=Dressel%2CH&author=H%C3%A4mmig%2CO&author=Bauer%2CGF)
26. Kahlert CR, Persi R, Güsewell S, Egger T, Leal-Neto OB, Sumer J, et al. Non-occupational and occupational factors associated with specific SARS-CoV-2 antibodies among hospital workers – a multicentre cross-sectional study. Clin Microbiol Infect. 2021;27:1336–44. <https://doi.org/10.1016/j.cmi.2021.05.014>.
[Article](https://doi.org/10.1016%2Fj.cmi.2021.05.014) [CAS](https://link.springer.com/articles/cas-redirect/1:CAS:528:DC%2BB3MXhtlegsbjF) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=34020033) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC8131187) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Non-occupational%20and%20occupational%20factors%20associated%20with%20specific%20SARS-CoV-2%20antibodies%20among%20hospital%20workers%20%E2%80%93%20a%20multicentre%20cross-sectional%20study&journal=Clin%20Microbiol%20Infect&doi=10.1016%2Fj.cmi.2021.05.014&volume=27&pages=1336-1344&publication_year=2021&author=Kahlert%2CCR&author=Persi%2CR&author=G%C3%BCsewell%2CS&author=Egger%2CT&author=Leal-Neto%2COB&author=Sumer%2CJ)
27. Federal Office of Public Health. Virus variants overview. \[Internet\]. \[cited 2025 Apr 21\]. <https://www.covid19.admin.ch/en/epidemiologic/virus-variants>. Accessed 21 Apr 2025.
28. Coronavirus: Key Decisions of the Federal Council \[Internet\]. \[cited 2025 May 2\]. <https://www.uvek.admin.ch/uvek/de/home/uvek/coronavirus/wichtige-entscheide.html>. Accessed 2 May 2025.
29. Kohler P, Güsewell S, Seneghini M, Egger T, Leal O, Brucher A, et al. Impact of baseline SARS-CoV-2 antibody status on syndromic surveillance and the risk of subsequent COVID-19—a prospective multicenter cohort study. BMC Med. 2021;19:270. <https://doi.org/10.1186/s12916-021-02144-9>.
[Article](https://link.springer.com/doi/10.1186/s12916-021-02144-9) [CAS](https://link.springer.com/articles/cas-redirect/1:CAS:528:DC%2BB3MXit1OiurzF) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=34649585) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC8514323) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Impact%20of%20baseline%20SARS-CoV-2%20antibody%20status%20on%20syndromic%20surveillance%20and%20the%20risk%20of%20subsequent%20COVID-19%E2%80%94a%20prospective%20multicenter%20cohort%20study&journal=BMC%20Med&doi=10.1186%2Fs12916-021-02144-9&volume=19&publication_year=2021&author=Kohler%2CP&author=G%C3%BCsewell%2CS&author=Seneghini%2CM&author=Egger%2CT&author=Leal%2CO&author=Brucher%2CA)
30. Klok FA, Boon GJAM, Barco S, Endres M, Geelhoed JJM, Knauss S, et al. The Post-COVID-19 Functional Status scale: a tool to measure functional status over time after COVID-19. Eur Respir J. 2020;56:2001494. <https://doi.org/10.1183/13993003.01494-2020>.
[Article](https://doi.org/10.1183%2F13993003.01494-2020) [CAS](https://link.springer.com/articles/cas-redirect/1:CAS:528:DC%2BB3cXitVCjtLfN) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=32398306) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC7236834) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=The%20Post-COVID-19%20Functional%20Status%20scale%3A%20a%20tool%20to%20measure%20functional%20status%20over%20time%20after%20COVID-19&journal=Eur%20Respir%20J&doi=10.1183%2F13993003.01494-2020&volume=56&publication_year=2020&author=Klok%2CFA&author=Boon%2CGJAM&author=Barco%2CS&author=Endres%2CM&author=Geelhoed%2CJJM&author=Knauss%2CS)
31. Fernandez-de-las-Peñas C, Notarte KI, Macasaet R, Velasco JV, Catahay JA, Ver AT, et al. Persistence of post-COVID symptoms in the general population two years after SARS-CoV-2 infection: a systematic review and meta-analysis. J Infect. 2024;88:77–88. <https://doi.org/10.1016/j.jinf.2023.12.004>.
[Article](https://doi.org/10.1016%2Fj.jinf.2023.12.004) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=38101521) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Persistence%20of%20post-COVID%20symptoms%20in%20the%20general%20population%20two%20years%20after%20SARS-CoV-2%20infection%3A%20a%20systematic%20review%20and%20meta-analysis&journal=J%20Infect&doi=10.1016%2Fj.jinf.2023.12.004&volume=88&pages=77-88&publication_year=2024&author=Fernandez-de-las-Pe%C3%B1as%2CC&author=Notarte%2CKI&author=Macasaet%2CR&author=Velasco%2CJV&author=Catahay%2CJA&author=Ver%2CAT)
32. Kim Y, Bae S, Chang H-H, Kim S-W. Long COVID prevalence and impact on quality of life 2 years after acute COVID-19. Sci Rep. 2023;13:11207. <https://doi.org/10.1038/s41598-023-36995-4>.
[Article](https://doi.org/10.1038%2Fs41598-023-36995-4) [CAS](https://link.springer.com/articles/cas-redirect/1:CAS:528:DC%2BB3sXhsVKksrzM) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=37433819) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC10336045) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Long%20COVID%20prevalence%20and%20impact%20on%20quality%20of%20life%202%20years%20after%20acute%20COVID-19&journal=Sci%20Rep&doi=10.1038%2Fs41598-023-36995-4&volume=13&publication_year=2023&author=Kim%2CY&author=Bae%2CS&author=Chang%2CH-H&author=Kim%2CS-W)
33. Nguyen NN, Tissot-Dupont H, Brouqui P, Gautret P. Post-COVID syndrome in symptomatic COVID-19 patients: a retrospective cohort study. BMC Infect Dis. 2025;25:1099. <https://doi.org/10.1186/s12879-025-11360-0>.
[Article](https://link.springer.com/doi/10.1186/s12879-025-11360-0) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=40903751) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC12406458) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Post-COVID%20syndrome%20in%20symptomatic%20COVID-19%20patients%3A%20a%20retrospective%20cohort%20study&journal=BMC%20Infect%20Dis&doi=10.1186%2Fs12879-025-11360-0&volume=25&publication_year=2025&author=Nguyen%2CNN&author=Tissot-Dupont%2CH&author=Brouqui%2CP&author=Gautret%2CP)
34. Danesh V, Arroliga AC, Bourgeois JA, Boehm LM, McNeal MJ, Widmer AJ, et al. Symptom clusters seen in adult COVID-19 recovery clinic care seekers. J Gen Intern Med. 2023;38:442–9. <https://doi.org/10.1007/s11606-022-07908-4>.
[Article](https://link.springer.com/doi/10.1007/s11606-022-07908-4) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=36376627) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Symptom%20clusters%20seen%20in%20adult%20COVID-19%20recovery%20clinic%20care%20seekers&journal=J%20Gen%20Intern%20Med&doi=10.1007%2Fs11606-022-07908-4&volume=38&pages=442-449&publication_year=2023&author=Danesh%2CV&author=Arroliga%2CAC&author=Bourgeois%2CJA&author=Boehm%2CLM&author=McNeal%2CMJ&author=Widmer%2CAJ)
35. Huiberts AJ, De Bruijn S, Andeweg SP, Hoeve CE, Schipper M, De Melker HE, et al. Prospective cohort study of fatigue before and after SARS-CoV-2 infection in the Netherlands. Nat Commun. 2025;16:1923. <https://doi.org/10.1038/s41467-025-56994-5>.
[Article](https://doi.org/10.1038%2Fs41467-025-56994-5) [CAS](https://link.springer.com/articles/cas-redirect/1:CAS:528:DC%2BB2MXlslSkurs%3D) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=40038286) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC11880519) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Prospective%20cohort%20study%20of%20fatigue%20before%20and%20after%20SARS-CoV-2%20infection%20in%20the%20Netherlands&journal=Nat%20Commun&doi=10.1038%2Fs41467-025-56994-5&volume=16&publication_year=2025&author=Huiberts%2CAJ&author=Bruijn%2CS&author=Andeweg%2CSP&author=Hoeve%2CCE&author=Schipper%2CM&author=Melker%2CHE)
36. Strahm C, Seneghini M, Güsewell S, Egger T, Leal-Neto O, Brucher A, et al. Symptoms compatible with long coronavirus disease (COVID) in healthcare workers with and without severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection—results of a prospective multicenter cohort. Clin Infect Dis. 2022;75:e1011–9. <https://doi.org/10.1093/cid/ciac054>.
[Article](https://doi.org/10.1093%2Fcid%2Fciac054) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=35090015) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC9383387) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Symptoms%20compatible%20with%20long%20coronavirus%20disease%20%28COVID%29%20in%20healthcare%20workers%20with%20and%20without%20severe%20acute%20respiratory%20syndrome%20coronavirus%202%20%28SARS-CoV-2%29%20infection%E2%80%94results%20of%20a%20prospective%20multicenter%20cohort&journal=Clin%20Infect%20Dis&doi=10.1093%2Fcid%2Fciac054&volume=75&pages=e1011-e1019&publication_year=2022&author=Strahm%2CC&author=Seneghini%2CM&author=G%C3%BCsewell%2CS&author=Egger%2CT&author=Leal-Neto%2CO&author=Brucher%2CA)
37. Nakagama Y, Komase Y, Kaku N, Nitahara Y, Tshibangu-Kabamba E, Tominaga T, et al. Detecting waning serological response with commercial immunoassays: 18-month longitudinal follow-up of anti-SARS-CoV-2 Nucleocapsid antibodies. Microbiol Spectr. 2022;10:e00986-22. <https://doi.org/10.1128/spectrum.00986-22>.
[Article](https://doi.org/10.1128%2Fspectrum.00986-22) [CAS](https://link.springer.com/articles/cas-redirect/1:CAS:528:DC%2BB38XisVyqt73M) [PubMed](http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=35867423) [PubMed Central](http://www.ncbi.nlm.nih.gov/pmc/articles/PMC9430644) [Google Scholar](http://scholar.google.com/scholar_lookup?&title=Detecting%20waning%20serological%20response%20with%20commercial%20immunoassays%3A%2018-month%20longitudinal%20follow-up%20of%20anti-SARS-CoV-2%20Nucleocapsid%20antibodies&journal=Microbiol%20Spectr&doi=10.1128%2Fspectrum.00986-22&volume=10&publication_year=2022&author=Nakagama%2CY&author=Komase%2CY&author=Kaku%2CN&author=Nitahara%2CY&author=Tshibangu-Kabamba%2CE&author=Tominaga%2CT)
[Download references](https://citation-needed.springer.com/v2/references/10.1007/s15010-026-02768-0?format=refman&flavour=references)
## Acknowledgements
The SURPRISE+ Study Group: Alexia Cusini, Cantonal Hospital Graubuenden, Chur, Switzerland; Tamara Dörr, HOCH, Cantonal Hospital St.Gallen, Division of Infectious Diseases, Infection Prevention and Travel Medicine, St.Gallen, Switzerland; Stephan Goppel, Psychiatry Services of the Canton of St Gallen, St Gallen, Switzerland; Fabian Grässli, HOCH, Cantonal Hospital St.Gallen, Division of Infectious Diseases, Infection Prevention and Travel Medicine, St.Gallen, Switzerland, Christian R. Kahlert; HOCH, Cantonal Hospital St.Gallen, Division of Infectious Diseases, Infection Prevention and Travel Medicine, St.Gallen, Switzerland and Department of InfectiousDiseases and Hospital Epidemiology, Children’s Hospital of EasternSwitzerland,St. Gallen, Switzerland; Joelle Keller, Hirslanden Clinic Zurich, Zurich, Switzerland; Simone Kessler, HOCH, Cantonal Hospital St.Gallen, Division of Infectious Diseases, Infection Prevention and Travel Medicine, St.Gallen, Switzerland; Philipp Kohler, HOCH, Cantonal Hospital St.Gallen, Division of Infectious Diseases, Infection Prevention and Travel Medicine, St.Gallen, Switzerland and Epidemiology, Biostatistics and Prevention Institute (EBPI), University of Zurich, Zurich, Switzerland; Stefan P. Kuster, HOCH, Cantonal Hospital St.Gallen, Division of Infectious Diseases, Infection Prevention and Travel Medicine, St.Gallen, Switzerland; J. Carsten Möller, Center for Neurological Rehabilitation Zihlschlacht, Zihlschlacht, Switzerland; Maja F. Müller, Hirslanden Clinic Zurich, Zurich, Switzerland; Philip Rieder, Hirslanden Clinic Zurich, Zurich, Switzerland; Lorenz Risch, Labormedizinisches Zentrum Dr Risch Ostschweiz AG, Buchs, Switzerland, Private Universität im Fürstentum Liechtenstein, Triesen, Liechtenstein and Center of Laboratory Medicine, Institute of Clinical Chemistry, University of Bern, Inselspital, Bern, Switzerland; Markus Rütti, HOCH, Hospital Wil, Division of Internal Medicine, St. Gallen, Switzerland; Matthias Schlegel, HOCH, Cantonal Hospital St.Gallen, Division of Infectious Diseases, Infection Prevention and Travel Medicine, St.Gallen, Switzerland; Reto Stocker, Hirslanden Clinic Zurich, Zurich, Switzerland and Foundation Quality of Life, Zurich, Switzerland; Matthias von Kietzell, Hirslanden Clinic Stephanshorn, St. Gallen, Switzerland; Danielle Vuichard-Gysin, Thurgau Hospital Group, Division of Infectious Diseases and Hospital Epidemiology, Muensterlingen and Frauenfeld, Switzerland; Department of Research and Development, Swiss National Centre for Infection Prevention (Swissnoso), Bern, Switzerland; Geriatric Clinic St. Gallen, St. Gallen, Switzerland.
## Funding
This work was supported by the Swiss National Sciences Foundation SNSF (grant number 31CA30\_196544; grant number PZ00P3\_179919 to PK).
## Author information
Author notes
1. Tamara Dörr and Philipp Kohler equal contribution as last authors.
### Authors and Affiliations
1. Division of Infectious Diseases, Infection Prevention and Travel Medicine, HOCH, Cantonal Hospital St.Gallen, Rorschacher Strasse 95, 9007, St. Gallen, Switzerland
Christian R. Kahlert, Stefan P. Kuster, Matthias Schlegel, Carol Strahm, Tamara Dörr & Philipp Kohler
2. Epidemiology, Biostatistics and Prevention Institute (EBPI), University of Zurich, Hirschengraben 84, 8001, Zurich, Switzerland
Philipp Saurer, Tala Ballouz, Sarah R. Haile, Milo A. Puhan & Philipp Kohler
3. Cantonal Hospital Graubuenden, Chur, Switzerland
Alexia Cusini
4. Hirslanden Clinic Stephanshorn, St. Gallen, Switzerland
Matthias von Kietzell
5. Division of Internal Medicine, HOCH, Hospital Wil, St. Gallen, Switzerland
Markus Rütti
6. Hirslanden Clinic Zurich, Zurich, Switzerland
Reto Stocker
7. Division of Infectious Diseases and Hospital Epidemiology, Thurgau Hospital Group, Muensterlingen, Frauenfeld, Switzerland
Danielle Vuichard-Gysin
8. Department of Research and Development, Swiss National Centre for Infection Prevention (Swissnoso), Bern, Switzerland
Danielle Vuichard-Gysin
9. Department of Infectious Diseases and Hospital Epidemiology, Children’s Hospital of Eastern Switzerland, St. Gallen, Switzerland
Christian R. Kahlert
10. Labormedizinisches Zentrum Dr Risch Ostschweiz AG, Buchs, Switzerland
Lorenz Risch
11. Private Universität im Fürstentum Liechtenstein, Triesen, Liechtenstein
Lorenz Risch
12. Center of Laboratory Medicine, Institute of Clinical Chemistry, University of Bern, Inselspital, Bern, Switzerland
Lorenz Risch
13. Foundation Quality of Life, Zurich, Switzerland
Reto Stocker
Authors
1. Philipp Saurer
2. Tala Ballouz
3. Alexia Cusini
4. Sarah R. Haile
5. Christian R. Kahlert
6. Matthias von Kietzell
7. Stefan P. Kuster
8. Markus Rütti
9. Matthias Schlegel
10. Carol Strahm
11. Reto Stocker
12. Danielle Vuichard-Gysin
13. Lorenz Risch
14. Milo A. Puhan
15. Tamara Dörr
16. Philipp Kohler
### Consortia
### on behalf of the SURPRISE+ cohort
- Alexia Cusini
- , Tamara Dörr
- , Stephan Goppel
- , Fabian Grässli
- , Christian R. Kahlert
- , Joelle Keller
- , Simone Kessler
- , Philipp Kohler
- , Stefan P. Kuster
- , J. Carsten Möller
- , Maja F. Müller
- , Philip Rieder
- , Lorenz Risch
- , Markus Rütti
- , Matthias Schlegel
- , Reto Stocker
- , Matthias von Kietzell
- & Danielle Vuichard-Gysin
### Contributions
All authors contributed to the study conception and design. Data collection was performed by the SURPRISE + Study Group. Data analyses were performed by P.S. The first draft of the manuscript was written by P.S. and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript. T.D. and P.K. contributed equally as last authors.
### Corresponding authors
Correspondence to [Philipp Saurer](mailto:philippdaniel.saurer@uzh.ch) or [Philipp Kohler](mailto:philipp.kohler@h-och.ch).
## Ethics declarations
### Conflict of interest
The authors declare no competing interests.
### Ethical approval
The study protocol was approved by the Ethics Committee of Eastern Switzerland (\#2020–00502).
### Consent to participate
All participants provided electronic informed consent.
## Rights and permissions
**Open Access** This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit <http://creativecommons.org/licenses/by-nc-nd/4.0/>.
[Reprints and permissions](https://s100.copyright.com/AppDispatchServlet?title=Persistence%20of%20Post-Acute%20COVID-19%20Sequelae%20%28PASC%29%20symptoms%20in%20healthcare%20workers%20four%20years%20after%20ancestral%20SARS-CoV-2%20infection%3A%20a%20prospective%20multicentre%20cohort&author=Philipp%20Saurer%20Stephan%20Goppel%20et%20al&contentID=10.1007%2Fs15010-026-02768-0©right=The%20Author%28s%29&publication=0300-8126&publicationDate=2026-03-17&publisherName=SpringerNature&orderBeanReset=true&oa=CC%20BY-NC-ND)
## About this article
[](https://crossmark.crossref.org/dialog/?doi=10.1007/s15010-026-02768-0)
### Cite this article
Saurer, P., Ballouz, T., Cusini, A. *et al.* Persistence of Post-Acute COVID-19 Sequelae (PASC) symptoms in healthcare workers four years after ancestral SARS-CoV-2 infection: a prospective multicentre cohort. *Infection* (2026). https://doi.org/10.1007/s15010-026-02768-0
[Download citation](https://citation-needed.springer.com/v2/references/10.1007/s15010-026-02768-0?format=refman&flavour=citation)
- Received: 22 December 2025
- Accepted: 10 March 2026
- Published: 17 March 2026
- Version of record: 17 March 2026
- DOI: https://doi.org/10.1007/s15010-026-02768-0
### Keywords |
| Shard | 129 (laksa) |
| Root Hash | 17645177711233004329 |
| Unparsed URL | com,springer!link,/article/10.1007/s15010-026-02768-0 s443 |